The 2024 San Antonio Breast Cancer Symposium (SABCS24) included 50 research posters focused on lobular breast cancer, more than double the number presented at last year’s event. The large posters presented on boards in the exhibit hall at research conferences are the tools scientists use to graphically present the overview, key findings and discussion from the abstracts they have created with the preliminary findings of their most recent research. After presentation of the abstracts at SABCS the scientists frequently then submit their research for publication in manuscripts. These abstracts will also be published in a special publication by the American Association of Cancer Research (AACR) in the Spring of 2025 .
Below is a collection of the summaries of most of the ILC research poster presentations from SABCS 2024 in simple language. Permission to share these posters and lay summaries has been granted by the authors.
List of Posters and Lay Summaries
List of Posters and Lay Summaries
- P1-03-08: Clinico-pathological Characteristics of Breast Invasive Lobular Carcinoma in non-CDH1 genetic predisposition. Experience from the Institut Curie
- P1-03-29: Targeted Human Plasma Metabolomics for Lobular Breast Cancer Biomarker Discovery
- P1-05-16: Differential ctDNA-based genomic features of Triple-Negative Metastatic Lobular Breast carcinoma: insights into a rare and poorly understood disease
- P1-05-29: The Nanomechanical Phenotype of Lobular Breast Cancer
- P1-08-20: Synchronic invasive lobular breast carcinoma, invasive mammary carcinoma NST, and large cell neuroendocrine carcinoma of the lung
- P1-10-21: Intrathecal therapy in invasive lobular carcinoma with non-bulky leptomeningeal disease: case report
- P1-11-14: Hormone receptor positive (ER+) HER2+ Lobular Breast Carcinoma: Molecular Response to Perioperative Endocrine Therapy and Clinical Outcomes in the POETIC Trial
- P2-07-24: Results from the Phase II Study of ROS1 Targeting with Crizotinib in Advanced E-cadherin Negative Lobular Breast Cancer (ROLo)
- P2-10-03: Real world outcomes of adjuvant chemotherapy in invasive lobular carcinoma of the breast: a retrospective cohort from a reference center in Brazil
- P3-05-19: High Prevalence of HER2-Low and Increased TIL Levels in ILC Patients with Residual Disease Following Neoadjuvant Therapy Provides a Rational for use of HER2-Antibody-Drug Conjugates or Immunotherapy Approaches
- P3-06-24: Characterization of a Living Biobank of Patient-Derived Invasive Lobular Carcinoma Organoids that Retain Tumor Heterogeneity in 3D Culture and Tumorigenicity In Vivo
- P3-09-18: Comparative analysis of protein and gene expression of biomarkers and therapeutic targets in patients with metastatic hormone-receptor positive breast cancer of no-special type versus invasive lobular breast cancer
- P3-09-23: Investigating differences in the composition of circulating tumor cells (CTCs) clusters in invasive lobular and ductal carcinoma to decipher lobular breast cancer metastasis
- P3-09-27: Identification of glucocorticoid receptor dependence in metastasis of invasive lobular carcinoma using an in vivo xenograft MIND model
- P4-01-16: Comprehensive Genomic Characterization of ILC Organoids: A BCRF Legacy Project Initiative
- P4-10-24: Extracellular matrix remodelling is a targetable feature of invasive lobular carcinoma (ILC)
- P5-02-29: Redefining PARP inhibitor paradigms to target DNA repair dysfunction in lobular breast cancer
- P5-04-05: Impact of racial and socioeconomic disparities on overall survival in Invasive Lobular Carcinoma
- P5-06-02: Comparison of lobular vs NST hormone receptor positive metastatic breast cancer patients in early lines of treatment via comprehensive genomic profiling and whole genome sequencing of circulating tumor DNA
- PS18-01: Spatial Transcriptomics-Derived Classification of Invasive Lobular Carcinoma: Associations with Clinical, Genomic Characteristics, and Prognosis
- PS18-02: E-cadherin inactivation shapes tumor microenvironment specificities in invasive lobular carcinoma
- PS18-03: GeoMx DSP and CosMx single cell spatial transcriptomics for molecular characterization of invasive lobular breast cancer cells and their microenvironment
- PS18-04: Tumor intrinsic and extrinsic characteristics of invasive lobular carcinomas
- PS18-07: Differential odds of response in ILC versus IDC correlate with changes in the TIME in a phase II trial of pre-operative fulvestrant with or without enzalutamide
- PS18-09: Endocrine Response in Women with Invasive Lobular Carcinoma (TBCRC 037): A Multicenter Randomized Clinical Trial
Lay Summaries and Posters:
The available research posters are linked in the titles below.
P1-03-08: Clinico-pathological Characteristics of Breast Invasive Lobular Carcinoma in non-CDH1 genetic predisposition. Experience from the Institut Curie
ILCs occurring in the context of constitutional genetic predisposition unrelated to CDH1 remain poorly characterized in the literature. We performed a single-center retrospective clinico-pathological study of ILCs associated with germline BRCA1 (N=17), BRCA2 (N=80) or PALB2 (N=12) mutations. ILC was the first cancer diagnosed in almost all patients and occurred at a younger age than sporadic ILCs. BRCA2– and PALB2-associated ILCs had similar histopathological features to sporadic ILCs. In contrast, BRCA1-associated ILCs showed a distinct phenotype (more grade 3 and HR-negative tumors), suggesting that BRCA1 mutations may drive the ILC phenotype, although this gene has not yet been identified as a predisposing factor for lobular carcinoma.
P1-03-29: Targeted Human Plasma Metabolomics for Lobular Breast Cancer Biomarker Discovery
Researchers have made an important discovery in the fight against lobular breast cancer (LBC), a type of breast cancer that can be difficult to diagnose. By analyzing blood samples from women with LBC, another type of breast cancer called invasive ductal carcinoma (IDC), and healthy individuals, they found unique metabolic “fingerprints” for each group.
The study revealed that a combination of just three metabolites (small molecules in the blood) and a person’s age could accurately identify women with LBC. This is exciting because it could lead to a new, less invasive way to diagnose LBC, which is often hard to detect with traditional methods like mammograms.
These findings are significant for several reasons. First, they could help doctors diagnose LBC earlier, which is crucial for better treatment outcomes. Second, understanding the unique metabolic characteristics of LBC might help scientists develop more targeted treatments. Finally, this research opens the door to more personalized care for women with LBC, potentially improving their chances of recovery and quality of life during treatment.
P1-05-16: Differential ctDNA-based genomic features of Triple-Negative Metastatic Lobular Breast carcinoma: insights into a rare and poorly understood disease
In this study, we investigated the genetic characteristics of triple-negative invasive lobular carcinoma (TN-ILC), a rare subtype of breast cancer that accounts for only 2% of all triple-negative (TNBC) diagnoses and less than 0.1% of all breast cancer cases. Due to its rarity, TN-ILC remains poorly understood and lacks well-defined treatment strategies, making it challenging to manage effectively.
Our research utilized a blood-based test known as circulating tumor DNA (ctDNA), which detects and analyzes fragments of DNA shed by cancer cells into the bloodstream. We examined ctDNA samples from 750 patients with metastatic breast cancer, collected between 2015 and 2023 from multiple institutions. The goal was to identify specific genetic alterations in TN-ILC and compare them to those found in more common subtypes, such as triple-negative invasive ductal carcinoma (TN-IDC) and hormone receptor-positive invasive lobular carcinoma (HRpos-ILC).
The analysis showed distinct genetic features in TN-ILC, particularly in key genes such as PIK3CA, TP53, ERBB2, and CDH1, which exhibited unique alteration patterns. For instance, mutations in PIK3CA were significantly more frequent in TN-ILC, while TP53 mutations were less prevalent. Additionally, TN-ILC showed greater involvement of specific signaling pathways, such as PI3K and RAS, compared to TN-IDC. Survival analysis demonstrated that TN-ILC had similarly poor overall survival to TN-IDC, with both subtypes showing worse outcomes than their hormone receptor-positive counterparts.
These findings highlight the need to better understand the genetic features of rare breast cancer subtypes like TN-ILC. A deeper understanding of these features could inform the development of personalized treatment strategies, improving therapeutic effectiveness while minimizing unnecessary toxicities.
P1-05-29: The Nanomechanical Phenotype of Lobular Breast Cancer
Invasive lobular breast cancer (ILC), also known as invasive lobular carcinoma, is increasingly recognized as a distinct type of breast cancer with unique biological and clinical characteristics. Unlike the more common invasive ductal carcinoma (IDC), ILC cells exhibit a characteristic “Indian file” pattern, where cancer cells are loosely arranged and lack strong connections to one another. ILC is often estrogen receptor-positive but can occur in all breast cancer subtypes. Research indicates that patients with ILC typically experience worse outcomes compared to those with IDC, including a higher risk of cancer metastasis and lower response rates to standard treatments. A key factor in the development of ILC is the loss of a protein called E-cadherin, which is crucial for maintaining cell-to-cell adhesion. This loss contributes to changes in the physical properties of the cancer cells and their surrounding environment, making the cancer more aggressive. These differences highlight the need for specialized approaches to diagnosing and treating ILC.
This study provides the first detailed analysis of the nanomechanical properties of ILC tissues, examining features such as tissue stiffness and adhesion through a novel diagnostic tool. The findings confirm that ILC has a unique mechanical profile compared to IDC, supporting the notion of treating it as a separate breast cancer subtype. The study also investigated the various subtypes and variants of ILC, revealing distinct stiffness patterns in both classic and non-classic ILC. These differences likely influence their growth, underscoring the importance of further research into tailored treatment options for each subtype. Ongoing research, including a large clinical trial, aims to deepen our understanding of ILC and enhance treatment strategies, ultimately leading to improved outcomes for patients facing this challenging type of breast cancer.
P1-08-20: Synchronic invasive lobular breast carcinoma, invasive mammary carcinoma NST, and large cell neuroendocrine carcinoma of the lung
In this rare clinical case, we describe our experience in managing synchronous bilateral invasive lobular cancer (ILC) in a postmenopausal patient. The patient initially identified a 23 mm nodule in the upper quadrant of the right breast during routine screening. Upon her arrival at our clinic, the lesion was confirmed as ILC, grade I, estrogen receptor (ER) positive, with a Ki-67 index of 14%. Further staging examinations revealed a second nodule in the left breast, measuring 56 mm in the inferomedial quadrant. Core biopsy confirmed this as a second ILC, grade II, ER positive. Additionally, imaging identified an irregular pulmonary nodule measuring 49 mm in the upper right lobe and an enlarged right hilar lymph node. A biopsy of the pulmonary nodule confirmed a third primary malignancy: large-cell neuroendocrine carcinoma (LCNEC).
This case was thoroughly reviewed in a multidisciplinary tumor board comprising a mastologist, thoracic surgeon, pathologist, radiologist, and oncologist. The treatment plan initiated neoadjuvant endocrine therapy for breast cancer. Given the poor prognosis associated with the lung cancer, priority was given to surgical resection of the pulmonary tumor. Following this, the patient underwent adjuvant chemotherapy. After three months, bilateral mastectomy was performed, followed by adjuvant radiotherapy, a cyclin-dependent kinase (CDK) inhibitor, and continued endocrine therapy.
This case underscores the importance of a multidisciplinary approach in the management of complex oncological cases, as it can significantly improve patient outcomes.
P1-10-21: Intrathecal therapy in invasive lobular carcinoma with non-bulky leptomeningeal disease: case report
Leptomeningeal disease (LMD) is a rare and serious complication of breast cancer, where cancer cells spread to the membranes surrounding the brain and spinal cord. It usually has a poor prognosis, with most patients surviving only a few months. This study presents the case of a 68-year-old woman with invasive lobular carcinoma, a specific type of breast cancer who developed LMD. Despite the severity of her condition, she lived significantly longer than average and had improvements in her symptoms after receiving specialized treatments, including intrathecal methotrexate (a form of chemotherapy delivered directly into the spinal fluid).
The patient’s treatment journey involved a combination of systemic and intrathecal therapies. Notably, after starting intrathecal methotrexate, her symptoms of double vision improved, and tests showed no cancer cells in her spinal fluid after nine cycles. Remarkably, she experienced no cancer relapse in her central nervous system and lived for 59 months after the LMD diagnosis, a substantial extension compared to typical outcomes. This extended survival and symptom relief highlight the potential for targeted therapies to improve outcomes in select patients.
This case emphasizes the importance of personalized treatment approaches for patients with invasive lobular carcinoma and LMD. It demonstrates that even with a poor prognosis, carefully selected therapies can provide meaningful benefits, such as extended survival and improved quality of life. These findings encourage further research to refine the criteria for identifying patients who might benefit from similar treatments, potentially offering hope to others with this challenging condition.
P1-11-14: Hormone receptor positive (ER+) HER2+ Lobular Breast Carcinoma: Molecular Response to Perioperative Endocrine Therapy and Clinical Outcomes in the POETIC Trial
Invasive Lobular Carcinoma (ILC) is a less common type of breast cancer, making up about 15% of all cases. It is rare for ILC tumors to overexpress a protein called HER2, so most research has focused on other subtypes, such as HER2-negative breast cancer. This study investigated ILC cases that are both estrogen receptor-positive (ER+) and HER2-positive (HER2+), examining their response to short-term endocrine treatments (such as aromatase inhibitors) and to combinations of chemotherapy and anti-HER2 therapies. The research used data from the POETIC trial, one of the largest studies on ER+ breast cancer, which evaluated the effect of short-term endocrine treatments given before surgery.
The results showed that ER+/HER2+ ILC tumors are biologically similar to the more common invasive ductal carcinoma (IDC) type, but with some unique differences. At baseline, ILC tumors had significantly lower levels of cell adhesion signatures (features that affect how cells stick together) compared to IDC tumors. Despite these differences, the overall survival rates for ILC and IDC patients were similar.
Interestingly, ILC tumors showed better early responses to aromatase inhibitors than IDC tumors. However, the HER2-enriched subtype within ILC predicted a poorer response to these treatments. Without additional therapies, such as chemotherapy and anti-HER2 drugs, some ILC patients were more likely to see their cancer return. For patients at high risk of recurrence, combining treatments was particularly effective in preventing cancer from coming back.
This study provides valuable insights into how ER+/HER2+ ILC behaves and responds to treatment. While the findings highlight the benefits of combination therapies, more research is needed due to the small number of ILC patients included in this study. This will help tailor treatments to better meet the needs of patients with this rare subtype of breast cancer.
P2-07-24: Results from the Phase II Study of ROS1 Targeting with Crizotinib in Advanced E-cadherin Negative Lobular Breast Cancer (ROLo)
The ROLo trial was designed to test whether crizotinib, a lung cancer drug targeting a gene called ROS1, is useful for lobular breast cancer. Laboratory work with crizotinib and similar ROS1 targeted drugs had shown very promising anti-cancer effects in lobular cancer cells and mouse models.
Patients with hormone-sensitive metastatic (secondary) lobular breast cancer who had already received at least one line of treatment for their secondary breast cancer were treated with a combination of fulvestrant (a hormonal injection) and crizotinib tablets and their response to treatment was assessed with regular CT scans. Patients with hormone insensitive (triple negative) lobular breast cancer who had received at least one line of chemotherapy for their secondary breast cancer were treated with crizotinib tablets alone. Twenty-seven patients with hormone-sensitive cancers and five with triple negative cancers took part in the study. Nausea, vomiting, diarrhoea, abdominal pain and abnormal liver function tests were common side effects of crizotinib combined with fulvestrant. Only one patient had a significant reduction in their cancer volume, and the average duration of cancer control was only 1.8 months. Patients with hormone sensitive cancers lived for an average of 17.7 months after starting the study treatment. Patients with triple negative cancers lived an average of just 4.4 months.
The trial did not confirm the laboratory results and we are currently looking at the blood tests and tumour samples from all the patients who took part in the study to see if we can find out why it didn’t work.
P2-10-03: Real world outcomes of adjuvant chemotherapy in invasive lobular carcinoma of the breast: a retrospective cohort from a reference center in Brazil
This study evaluated the outcomes of patients with invasive lobular carcinoma (ILC) treated at a referral center in Brazil. We focused on the survival outcomes of adjuvant chemotherapy, neoadjuvant chemotherapy, or omission of chemotherapy in patients with early-stage ILC (stages I–III). A total of 153 patients diagnosed between 2015 and 2020 were included. Among them, 50% received adjuvant chemotherapy, 10% underwent neoadjuvant chemotherapy, and 40% did not receive chemotherapy. The analyses compared disease-free survival (DFS) and overall survival (OS) among these groups.
Patients who received adjuvant chemotherapy had the best OS, at 13.3 years, compared to 5.5 years in the neoadjuvant group and 7.5 years in the no-chemotherapy group. For stage I patients, outcomes were similar across groups. However, adjuvant chemotherapy was associated with improved survival in stages II and III. Certain factors were linked to a higher mortality risk: (1) Age increased the risk of death by 7% per year; (2) Each stage progression raised the risk of death by 4.2 times; (3) HER2+ lobular tumors were associated with a ninefold increase in mortality risk. Furthermore, neoadjuvant chemotherapy was associated with low response rates, as 88% of patients in this group underwent mastectomy.
Although our findings are not conclusive due to the retrospective nature of the study, they demonstrate the low response of ILC to neoadjuvant chemotherapy, which may have a detrimental effect on survival by delaying surgery. Why do these results matter? Currently, guidelines such as the NCCN recommend neoadjuvant chemotherapy for stages II, and III, and inflammatory tumors, following a similar approach to ductal carcinomas.
P3-05-19: High Prevalence of HER2-Low and Increased TIL Levels in ILC Patients with Residual Disease Following Neoadjuvant Therapy Provides a Rational for use of HER2-Antibody-Drug Conjugates or Immunotherapy Approaches
This study investigated the prevalence and implications of HER2-Low status and tumor-infiltrating lymphocytes (TILs) in invasive lobular carcinoma (ILC), and their possible correlation with other clinicopathologic features predictive of outcome in patients with residual disease after presurgical therapy. HER2-Low breast cancers have a HER2 immunohistochemical stain score of 1+ or 2+ with a negative fluorescence in situ hybridization (FISH) test. The prevalence and treatment implications of HER2-Low expression in ILC are poorly characterized. Patients with ILC who are selected for presurgical chemotherapy or presurgical endocrine therapy have primary tumor characteristics associated with more aggressive disease. The percentage of patients with no tumor remaining after either type of neoadjuvant therapy in patients with ILC is significantly lower than rates observed in no special type (ductal) carcinomas. Higher TIL levels in ILC have been previously correlated with decreased survival. Recent clinical trials have demonstrated significant clinical benefit from novel HER2 antibody-drug conjugates to treat HER 2-Low breast cancer in the metastatic setting.
Among 196 women with ILC treated at our institution, 37 received presurgical therapy. Thirteen received presurgical chemotherapy and 24 received presurgical endocrine therapy. Twenty-three (62%) were HER2-Low. The majority were clinical stage II-III (cT2/cT3), multifocal and lymph node-positive. HER2-Low tumors were associated with higher TILs and the presence of tertiary lymphoid structures compared with HER2-0 tumors (defined as absent HER2 expression or 1+ expression in < 10% of tumor cells). Tertiary lymphoid structures are dense aggregates of lymphocytes with follicle formation, resembling the reactive follicles seen in a lymph node, and presumed to be evidence of an immune response to tumor. All patients had residual disease and 95% had a large volume of tumor.
High prevalence of HER2-Low associated with higher TIL levels among ILC patients with residual disease following presurgical therapy suggests treatment resistance and provides for possible therapeutic opportunities with HER2 antibody-drug conjugates and/or immunotherapy-based approaches for these select patients.
P3-06-24: Characterization of a Living Biobank of Patient-Derived Invasive Lobular Carcinoma Organoids that Retain Tumor Heterogeneity in 3D Culture and Tumorigenicity In Vivo
Breast cancer (BC) is one of the primary causes of cancer related deaths among women worldwide. According to Cancer Statistics, over 310,720 new breast cancer diagnoses are expected in the United States in 2024 with an estimate of over 42,250 expected BC related deaths. Invasive Lobular Carcinoma (ILC) accounts for the 2nd most frequently diagnosed histological subtype of BC, constituting 10%-15% of all reported cases. ILC is hormonally driven (estrogen and progesterone receptors) with a hallmark characteristic of ILC being lack of E-cadherin (CDH1) expression or with mutations in the CDH1 gene reported in over 90% of cases. Mutations in the CDH1 gene have also been associated with 39%–52% increased lifetime risk of developing breast cancer in women. Current protocols for ILC treatment do not fully account for comprehensive ILC-specific features in the as compared to other BC subtypes, thus an in-depth molecular investigation is needed to understand ILC biology better and to facilitate the identification of novel therapeutic targets whose manipulation can positively influence
patient outcomes.
Recent research advances have shown that resected patient tumor samples can be grown in the laboratory as “mini-tumors”, called patient-derived organoids (PDOs), which are representative of the original tumor tissue composition, architecture, and can recapitulate many tumor/microenvironment interactions. Thus far such characterized models have not been available to investigate ILC biology.
Here, we describe the establishment and comprehensive characterization of a diverse biobank of ILC PDOs. We have performed in-depth genomic (mutational and copy number variation analysis), transcriptomic (RNA gene expression signatures) and histologic profiling (to test for the presence of estrogen and progesterone receptors) of the established ILC PDOs and validated the models to be true representatives of ILC. Comprehensive genomic profiling of ILC PDOs using a custom 143 cancer driver gene panel identified ILC specific mutations in the CDH1,
PIK3CA, TBX3, RUNX, etc. genes in PDOs. Analysis of altered chromosome composition identified widely reported chromosomal gains and losses (gains on Chr1q and losses on Chr16q and Chr17p among others) in established ILC PDOs. Transcriptomic profiling performed on matched tumor-normal pairs revealed the upregulation of ESR1 signalling-related pathways as well as enrichment of ESR1 target genes which are known to drive ILC carcinogenesis. Lastly, we also show that the established ILC PDOs when placed either into mammary glands or intra-ductally of NOD-SCID gamma mice retain their tumorigenicity in vivo and exhibit a single file growth pattern, characteristic of invasiveness in ILC tumors.
In summary, we have established a living biobank of ILC PDOs, often with matched normals (adjacent and/or distal), that are representative of different subtypes of ILC (classic, pleomorphic, tubule-lobular, mixed, etc.). Overall, this study has optimized a pipeline for establishment, culturing and validation of ILC PDOs as robust models to study ILC biology and identify specific therapeutic targets with a focus translational and personalized medicine.
P3-09-18: Comparative analysis of protein and gene expression of biomarkers and therapeutic targets in patients with metastatic hormone-receptor positive breast cancer of no-special type versus invasive lobular breast cancer
Of all patients with breast cancer, approximately 85% are diagnosed with invasive breast cancer of no-special type (IBC-NST) and 15% with invasive lobular breast cancer (ILC). IBC-NST and ILC are most often hormone receptor-positive (estrogen receptor (ER) and progesterone receptor (PR)) and HER2-negative, however these two subtypes have distinct characteristics. Compared to IBC-NST, ILC is characterized by: older age at diagnosis, less immune infiltration (depicted by stromal tumor-infiltrating lymphocytes (sTIL)), diffuse metastatic pattern with often involvement of organs less commonly invaded in metastatic breast cancer i.e. more often metastases in the digestive tract, … Although different characteristics, the treatment is the same for both subtypes. However, there is a lack of dedicated research to metastatic ILC.
Here, we aimed at comparing the expression levels of clinically relevant biomarkers (sTIL, ER, PR, HER2) on the protein level and antibody-drug conjugate targets and immune checkpoint markers on the transcriptomic level in metastatic ILC versus metastatic IBC-NST. We therefore included all metastases from 16 patients with metastatic IBC-NST and 9 patients with metastatic ILC within our post-mortem tissue donation cohort, UPTIDER (Leuven, Belgium, NCT04531696).
We observed that metastases in organs less often involved metastatic BC (e.g. stomach) are confirmed in patients with metastatic ILC. As described in primary, ILC metastases show less immune infiltration (sTIL) compared to IBC-NST metastases. Analysis of the phenotype of the different cells from the tumor microenvironment still needs to be done. Hormone receptor expression “change” from positive to negative is present in both subtypes in the metastatic setting. There was no significant difference in the receptor expression between IBC-NST and ILC metastases. All patients with ILC had at least one HER2-low metastasis and HER2-ultralow metastasis, which is relevant given the recent approval of anti-HER2 ADC in these immunohistochemical scoring categories. Amongst the targets for the currently approved or investigated antibody-drug conjugates or immune checkpoint inhibitors, there were no significant expression differences between both subtypes,
Post-mortem tissue donation enables us to unravel differences between metastatic ILC and metastatic IBC-NST by allowing extensive sampling of all metastases. Metastatic ILC shows a diffuse metastatic pattern and less immune infiltration compared to IBC-NST. Although no other significant differences were observed, further research is warranted in order to refine the treatment of patients with metastatic ILC.
P3-09-23: Investigating differences in the composition of circulating tumor cells (CTCs) clusters in invasive lobular and ductal carcinoma to decipher lobular breast cancer metastasis
Invasive lobular carcinoma (ILC) is the second most common breast cancer subtype, and it is a different entity than ductal breast cancer (IDC). However, patients are treated the same way regardless of histology, highlighting an urgent need for a deeper understanding of ILC and the development of specific treatments to improve patient outcomes.
Liquid biopsies – blood tests that detect tumor cells or DNA that are circulating in the bloodstream – offer a non-invasive approach to study cancer. They provide valuable insights into tumor characteristics and reduce the need for invasive tissue biopsies, particularly in cases where traditional biopsies are challenging. Despite their potential, liquid biopsy studies focusing exclusively on ILC are limited. Some studies have shown that patients with metastatic lobular breast cancer have a higher number of circulating tumor cells (CTCs), which are cells that detach from the primary tumor and circulate in the bloodstream. Interestingly, these cells tend to form clusters more often in ILC than in IDC, which is paradoxical given that ILC typically has impaired cell-cell adhesion, a key factor in cluster formation.
The aim of our study was to investigate whether distinct mechanisms are responsible for CTC clustering in ILC and IDC. We analyzed blood samples from 351 patients with metastatic lobular or ductal breast cancer to assess the features of CTC clusters in term of number, size (i.e., the number of aggregated cells), and the presence of white blood cells (WBCs). We found that although patients with ILC had more CTC clusters compared to those with IDC, the clusters in ILC were smaller and more often included WBCs. This suggests that immune cells may play a key role in cluster formation in ILC, potentially protecting tumor cells in circulation. Since CTC clusters are considered the primary seeds for metastases, understanding their formation mechanisms could lead to new treatment strategies. Additionally, our study revealed that higher numbers of CTC clusters in the bloodstream were associated with poorer survival, suggesting that CTC clusters may also serve as a valuable prognostic marker.
P3-09-27: Identification of glucocorticoid receptor dependence in metastasis of invasive lobular carcinoma using an in vivo xenograft MIND model
Estrogen receptor (ER)-positive, invasive lobular carcinoma (ILC) is the second most common histological subtype of breast cancer. Although the five-year stage-matched survival is improved compared to infiltrating ductal carcinoma (IDC), ILC late metastatic recurrences (>5 years) are more frequent to bone and brain. Understanding the molecular mechanisms of lobular breast cancer’s significantly dormant yet ultimately metastatic phenotype is important to improve clinical outcomes. By examining gene expression following glucocorticoid receptor (GR) activation in metastasis-derived ER+/GR+ human ILC cell lines, we recently uncovered that GR-activation increases integrin expression which may underlie increased GR positive ILC metastasis. Similarly, circulating tumor cells are highly prevalent in lobular carcinoma making it a good model for studying metastasis using the established in vivo xenograft MIND model. We hypothesized that tumor cell GR status may help drive metastasis to secondary organs such as bone and brain. Utilizing in vivo models with ILC cell lines for collection of brain, liver, lung, and femurs at 60, 90, 150 days we can better understand the role of tumor cell GR in early colonization at metastatic sites. Here, we show the presence of tumor cells within the vascularized regions of intact femurs using highly specialized microscopic and tissue clearing techniques. Future studies will include the use of GR modulators in the MIND model to test whether the modulators alter early colonization of GR positive ILC cells.
P4-01-16: Comprehensive Genomic Characterization of ILC Organoids: A BCRF Legacy Project Initiative
Invasive Lobular Carcinoma (ILC) is a unique subtype of breast cancer that accounts for 10-15% of all breast cancers. Unlike other breast cancer types, ILC grows in a distinct pattern, making it difficult to study and treat effectively. Our project aims to address this challenge by developing advanced organoid models—tiny 3D structures grown from patient tumor tissues that mimic the behavior of cancer in the body.
So far, we have successfully established nine ILC organoids, which serve as valuable tools for studying this cancer type. These organoids are undergoing advanced genetic analyses, including whole-exome sequencing (WES), RNA sequencing (RNA-seq), and single-cell sequencing, to better understand their unique genetic features. Additionally, we have performed similar analyses on patient tumor tissues to compare and validate the findings from the organoids.
Our research highlights the genetic diversity of ILC and provides new insights into how these tumors behave. By making these organoid models and their associated data available to the research community, we hope to accelerate discoveries that will lead to better treatments and improved outcomes for patients with ILC.
P4-10-24: Extracellular matrix remodelling is a targetable feature of invasive lobular carcinoma (ILC)
Invasive lobular carcinoma (ILC) cells are seen to interact closely with structural proteins like collagens and elastin in the tumour microenvironment. Specifically, ILC’s have increased expression of LOXL1, an enzyme which alters collagen structure to promote cancer spread. A new drug, PXS-5505, which inhibits LOXL1 activity, has shown promise in disrupting this process in other cancers, and is known to be safe for patients. This study investigated whether PXS-5505 could also be an effective treatment for ILC.
Using mouse models that mimic ILC progression, we tested PXS-5505 both alone and in combination with a treatment that reduces oestrogen levels, reflecting standard hormone therapy. The drug alone significantly reduced tumour growth and altered the collagen structure in the tumour environment, resulting in less aggressive cancer cell behaviour. In some ILC models, PXS-5505 was effective as a standalone treatment, while in others, it worked best when combined with hormone therapy. Additionally, the drug reduced cancer spread to the lungs in a model of aggressive ILC. At the molecular level, PXS-5505 decreased the expression of proteins involved in cell growth, adhesion, and survival.
These findings suggest that targeting how ILC cells interact with the structural proteins that support tumour growth, in combination with existing therapies, may prove beneficial for patients. Further clinical studies in ILC patients are needed to confirm these promising results.
P5-02-29: Redefining PARP inhibitor paradigms to target DNA repair dysfunction in lobular breast cancer
Invasive lobular carcinoma (ILC) lacks targeted therapy options, and patients with ILC are typically ineligible for a class of targeted therapies called PARP inhibitors (PARPi), since ILC rarely present with the “BRCA-like” phenotype linked to hereditary BRCA1/2 mutations. However, in ILC cells, we identified an interaction between estrogen receptor α (ER) and a key DNA repair protein (MDC1), which we linked to dysfunctional DNA repair. This dysfunction is similar to but distinct from “BRCA-like” DNA repair deficiency observed with BRCA1/2 mutations, and suggests that ILC cells may be sensitive to PARPi. In laboratory models, compared to ductal carcinoma cell lines, ILC cells show a unique sensitivity to the FDA-approved PARPi Talazoparib; the cells are durably growth-inhibited even after drug removal. In animal models of ILC, we find that three ER+ ILC tumor models are sensitive to combined estrogen deprivation (modeling aromatase inhibitors / AI) + Talazoparib, which is superior to AI alone in all three models. Together, our work shows that ILC cells and tumor models show a previously unappreciated form of PARPi sensitivity, which may support a novel precision treatment approach for patients with ILC.
P5-04-05: Impact of racial and socioeconomic disparities on overall survival in Invasive Lobular Carcinoma
Racial and socioeconomic differences are important factors linked to worse outcomes in cancer patients. Most previous studies on breast cancer focused on invasive ductal carcinoma (IDC) or included all breast cancer types together, in which majority of the cases are IDC. However, invasive lobular carcinoma (ILC) has characteristics different from IDC and has unique survival patterns. As a result, we still don’t know much about how racial and socioeconomic factors affect the survival of ILC patients.
In this study, we analyzed data from over 33,000 ILC patients to identify how these factors influence overall survival. After accounting for various clinical, racial, and socioeconomic factors known to be related to prognosis by using statistical method, we found that having a lower income or being unmarried were associated with shorter survival. Interestingly, race and geographical location did not significantly affect survival in ILC.
Our findings highlight the importance of providing financial and social support to improve survival outcomes for patients with ILC.
P5-06-02: Comparison of lobular vs NST hormone receptor positive metastatic breast cancer patients in early lines of treatment via comprehensive genomic profiling and whole genome sequencing of circulating tumor DNA
Circulating tumor DNA (ctDNA), which is DNA shed from the tumor into the bloodstream, allowsreal-time monitoring of the cancer’s progression and resistance patterns.
In this study, authors have compared levels and profiles of lobular carcinoma with non specific type. 107 patients were included, 20 with lobular carcinoma and 87 with non specific type. Levels of ctDNA as well as specific changes were analyzed. Distinct features can be observed between the two types of cancer and are promising for further deeper biological analyses of lobular carcinoma from ctDNA.
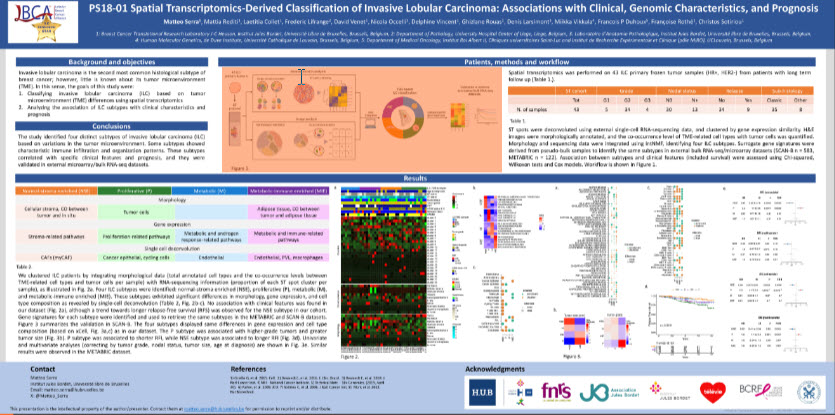
PS18-01: Spatial Transcriptomics-Derived Classification of Invasive Lobular Carcinoma: Associations with Clinical, Genomic Characteristics, and Prognosis
{kind=link}
Invasive lobular carcinoma (ILC) is the second most common histological sutype of breast cancer. This study identified four different subtypes of ILC by analyzing the diversity in the tumor’s surrounding environment. The tumor microenvironment is the set of normal cells, vessels and molecules that surround and feed tumor cells. These subtypes were found to be connected to different clinical characteristics and patient outcomes. We used spatial transcriptomics, a technique that looks at gene activity across different areas of a tumor, on 43 ILC samples. We grouped the patients into four categories: 1. Proliferative (P) – characterized by fast-growing tumor cells, 2. Normal-stroma enriched (NSE) – with a higher presence of supporting tissues and early-stage cancer cells, 3. Metabolic (M) – with cells involved in metabolism and blood vessels, 4. Metabolic-immune enriched (MIE) – with a mix of fat cells, immune cells, and blood vessels. In our cohort, those newly identified tumor microenvironment-based molecular subtypes were independent of histological subtypes (such as pleomorphic, mixed etc.). These subtypes were then confirmed in two larger datasets. The Proliferative subtype was associated with more aggressive features, like larger tumor size, higher tumor grade, and greater lymph node involvement, leading to poorer outcomes. In contrast, the Normal-stroma enriched subtype was linked to smaller tumors and better prognosis. These findings could help improve predictions of patient outcomes in ILC based on the tumor’s specific environment.
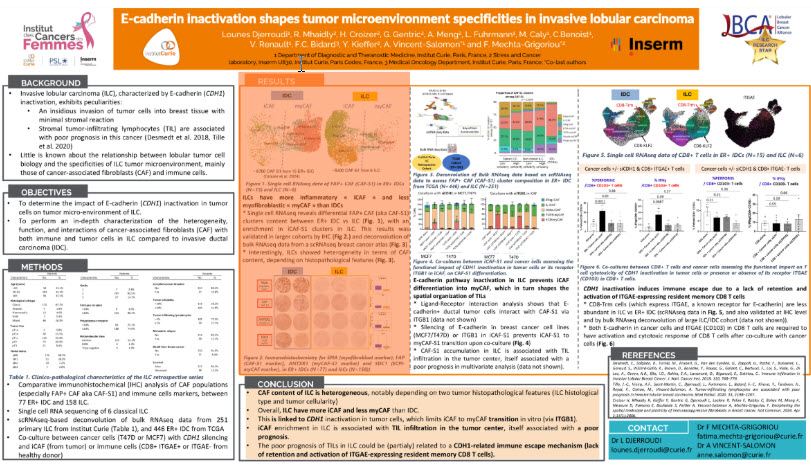
PS18-02: E-cadherin inactivation shapes tumor microenvironment specificities in invasive lobular carcinoma
{kind=link}
The tumor microenvironment (TME) is composed of a variety of cells that surround and interact with cancer cells in tumors. This ecosystem is now recognized as a key player in metastatic dissemination, anti-cancer immunity and response to anti-cancer treatments. Several observations by pathologists and researchers have suggested that the TME of ILC may have very different characteristics from those of other breast cancers. In this context, our team carried out a detailed characterization of the TME of ILC, in particular based on single-cell analyses. We identified the different types of fibroblasts and immune cells (the main components of the TME), their molecular composition and their spatial distribution in ILC compared to invasive ductal carcinoma. We discovered for the first time that the main genetic alteration in lobular tumor cells (E-cadherin inactivation) has a major impact on fibroblast maturation. In addition, E-cadherin alteration may allow lobular cells to escape from the immune system. Our findings provide a better understanding of the specificities of lobular disease and pave the way for new treatment strategies targeting TME.
PS18-03: GeoMx DSP and CosMx single cell spatial transcriptomics for molecular characterization of invasive lobular breast cancer cells and their microenvironment
Our recent studies in cell lines and mouse models have led us to hypothesize that activation of the stress hormone, glucocorticoid receptor (GR), reduces cellular proliferation but promotes migration of ILC cells hence leading to metastasis (Porter et al 2023). Human ILC tumor cells exhibit wide variation in nuclear GR expression, ranging from negative to strongly positive. We previously reported better patient outcome in ER+ breast cancers with high GR expression (Pan et al 2011) and we hypothesize that GR expression may impact the biology of ILC. We therefore used an integrated approach to explore the molecular profile of primary GR-positive vs. GR-negative ILC tumors from patients and to study interactions between tumor cells and neighboring cells within the tumor tissue. We measured average gene and protein expression in ILC tissue sections using GeoMx® digital spatial sequencing for genes and proteins, then CosMx™ single-cell spatial gene expression for a subset of those tumors.
We found that GR-positive ILC cells exhibited significant differences in gene and protein expression including downregulation of antigen presentation pathways that are important to enable the immune system to recognize and kill tumor cells. The most significantly enriched functional pathways in GR-negative tumor cells and surrounding non-tumor cells were those involved in forming and adapting the matrix that supports the tumor cells.
Single cell gene expression analysis confirmed lower expression of antigen presentation genes in the GR-positive tumor cells and fewer antigen presenting cells located around them. Single cell gene expression also revealed a higher abundance of a type of cancer-associated fibroblast (CAF) in close proximity to GR-negative tumor cells than to GR-positive ILC. Collectively, our data supports repression of antigen presentation pathways in GR-positive ILC accompanied by a relative exclusion of cancer-associated fibroblasts. Evidence suggests that tumor cells as well as stromal cells contribute to the formation of the supportive matrix, and that crosstalk between them leads to the establishment of a favorable environment to support ILC tumor cell survival, growth and invasion.
PS18-04: Tumor intrinsic and extrinsic characteristics of invasive lobular carcinomas
Invasive lobular carcinoma (ILC) is recognized as a unique type of breast cancer, distinct from other forms like invasive ductal carcinoma (IDC). Research shows that patients with ILC face a higher risk of cancer recurrence compared to the more common IDC form of breast cancer. Previously, in patients with either ILC or IDC disease, we identified molecular subgroups and associated biomarkers that can predict cancer recurrence. Our study aims to better understand the factors that contribute to the ILC-specific risk of relapse by analyzing the genomic (tumor intrinsic) and tumor physical environment (tumor extrinsic) characteristics of ILC tumors.
In this new study, we examined a large collection of primary breast cancer samples, revealing that patients with ILC have a greater chance of recurrence compared to those with IDC persistent even decades after their initial diagnosis. Importantly, this higher risk is independent of their molecular subtypes. In fact, we found that ILC tumors generally had stable genomes and displayed all the common good-prognosis molecular markers besides E-cadherin loss which contributes to tumor cell invasion. However, they were associated with a less active immune environment and a higher fraction of fibroblast cells in the tumor local environment. Interestingly, ILC cases display higher levels of communication between cancer and fibroblast cells. This type of cell-cell interaction might favor disease progression as shown in other cancer types. These findings suggest that ILC may require different treatment approaches, emphasizing the need for personalized therapy based on the specific traits of the tumor. By understanding the unique features of the ILC disease, we can work towards more effective strategies to manage this challenging disease.
PS18-07: Differential odds of response in ILC versus IDC correlate with changes in the TIME in a phase II trial of pre-operative fulvestrant with or without enzalutamide
The majority of estrogen receptor alpha positive (ER+) breast cancers are also positive for androgen receptors (AR). Since our published studies indicated that androgens can support the survival and progression of BC, we hypothesized that treatment with an anti-androgen used for treatment of prostate cancer would increase the percentage of patients with limited residual tumor at time of surgery as measured by modified preoperative endocrine predictive index (PEPI) score when combined with standard targeting of ER. Here, in a randomized phase II trial for women with large ER+/HER2- primary breast cancer (T2 or greater), the ER degrader fulvestrant (Fulv) was given either alone or in combination with the anti-androgen enzalutamide (Combo) for 4 months prior to surgery. A total of 59 patients were evaluable: 33 on Combo and 26 on Fulv. PEPI=0 (the best response) was achieved more frequently on the Combo arm (8/33) than Fulv only arm (2/26), although this difference (p=0.16) did not meet the pre-specified statistical significance (p=0.08). No new toxicities were experienced, most grade 1 with some mild reversible cognitive impairment and occasional tremor associated with enzalutamide.
Laboratory analyses of tumor biopsies at baseline, week 5 of treatment and tumors removed after 4 months of treatment showed that ER, and Ki67 levels decreased by W5 and time of surgery in both arms, whereas AR significantly decreased by time of surgery only in the Combo arm. AR and several growth factor receptors were among the proteins most differentially decreased by treatment in PEPI=0 tumors. Interestingly, the odds of response were 4.6-fold (95% CI: 0.9-22) higher for patients with ILC versus IDC. We examined active proteins that changed with treatment in ILC versus IDC and found that AR decreased significantly more with treatment in ILC versus IDC as did cell cycle proteins, growth/survival and metabolism proteins. Estrogen response and cell division gene sets decreased in tumors from both arms; however, Combo treated tumors uniquely exhibited enrichment of immune activation genes sets, including interferon gamma, complement, inflammation, antigen processing, and B and T cell activation. Furthermore, several types of immune suppressive cells were significantly decreased only in the Combo treated tumors and the number of tertiary lymphoid structures (TLS) per area surrounding surgical tumor resection, an indicator of an active immune system, was higher in the Combo arm compared to Fulv only arm and was significantly higher adjacent to tumors that achieved the best response PEPI=0 (P<0.03). Additionally, the average number of TLS/mm2 was higher in ILC versus IDC (P < 0.059) and several types of immune suppressive cells were uniquely reduced in the Combo arm (p<0.0002) and in responsive tumors (p<0.004).
We conclude that anti-androgens may be particularly useful for patients with ILC, although future studies with larger patient numbers would need to be conducted to confirm these results. And we need more studies with larger patient numbers to confirm these results.
PS18-09: Endocrine Response in Women with Invasive Lobular Carcinoma (TBCRC 037): A Multicenter Randomized Clinical Trial
Adjuvant endocrine therapy (ET) recommendations for patients with invasive lobular carcinoma (ILC) are no different than for other breast cancer subtypes. However, due to unique differences in estrogen pathway signaling of ILC, identifying biological markers of endocrine therapy sensitivity or resistance could have a major impact on its clinical management. Pre-clinical studies suggest that fulvestrant may be more effective than anastrozole or tamoxifen for ILC. Between 2015 and 2023, an open label, randomized, multicenter phase 0 window study was conducted at 12 TBCRC institutions to evaluate whether a biomarker of proliferation, Ki67, could be used to indicate treatment response to endocrine therapy.
Study participants were postmenopausal women with previously untreated hormone receptor-positive (HR+), HER2 negative ILC, with tumors measuring ≥ 1 cm. Stage IV was excluded. Patients were randomized 1:1:1 to receive fulvestrant, anastrozole, or tamoxifen prior to surgery. After 21-27 days of treatment, patients underwent surgery. The primary data point of interest in this study was change in Ki67 (measured by pathology immunohistochemistry of the tumor) at post-treatment compared to baseline. 201 women were randomized, 172 completed the assigned treatment, and 138 (fulvestrant n=37; anastrozole n=49; tamoxifen n=52) had evaluable pre- and post-treatment tissue. After statistical analyses were performed, there was a statistically significant difference in the reduction of Ki67 favoring fulvestrant vs. tamoxifen. There was not a significant difference in the reduction of Ki67 between anastrozole and tamoxifen, or between fulvestrant and anastrozole. The fact that tamoxifen resulted in a reduction of Ki67 similar to that of anastrozole, despite clinical concerns about its reduced efficacy in ILC, is an interesting finding. Next steps include further studies to determine whether Ki67 is associated with changes in the estrogen receptor and ER-regulated genes and/or in other novel pathways, which could potentially open new avenues for improved treatment strategies for ILC.
Why is this study important: This study helps improve our understanding of how ILC may respond to different endocrine therapies, what biomarkers can help to identify this, and what mechanisms are involved with potential changes in the tumor biology over time.