In December 2024, LBCA launched a patient experience survey focused on ILC breast cancer patients and the monitoring (referred to as “surveillance”) typically done to detect a recurrence or in the case of someone with metastatic ILC, a progression of their metastases. We are grateful for all who participated in this survey for your willingness to share your experiences.
We collect information from the many individual patients with ILC around the world, so that we can amplify our shared experiences and concerns with one voice in forums where we hope it will matter. We are so pleased that we were able to do so once again in presenting your important ILC patient experience messages to the scientists and clinicians attending the annual San Antonio Breast Cancer Symposium earlier this month. By bringing the ILC patient voice to this conference we alert the breast cancer treaters and researchers of the key challenges that ILC patients face that they should be aware of and will hopefully address. The following is what we heard from you in this survey and that we have shared in our poster presentation of results.
Survey Objectives
We aimed to survey a large number of ILC patients to capture what surveillance methods are being used and patient confidence that their surveillance plans – based on current protocols – will detect recurrences or progressions. As we anticipated, the survey results showed significant concern about the efficacy of surveillance plans for patients with ILC. Below we provide an overview of our survey respondents and findings.
Survey Results
1706 individuals with ILC or mixed ILC and other breast cancer subtypes completed our surveillance survey last year. Respondents were: 70% from the US, 11% from the UK, 6% from Australia, 5% from Canada, and 8% from 26 other countries. 12% of respondents are living with metastatic ILC and 88% reported having had early stage ILC (Stage I-II). Of those currently living with metastatic ILC, 40% had an initial ILC diagnosis of stage IV or metastatic ILC (referred to as “de novo” metastatic) and 60% were diagnosed with a distant recurrence.
Understanding that there are health system differences between the US and countries outside of the US, data were separated along these lines. Similarly, data were stratified and we analyzed the data from those with early stage and those living with metastatic ILC separately. While there were some differences in imaging and blood tests performed in the US and outside of the US, most rates were generally comparable (see the poster for more details). What stood out in the results were the high rates of lack of confidence in the surveillance plan.
We asked each respondent to provide written comments to explain their answers. Some of the key analyses we have already conducted on these descriptive responses are as follows.
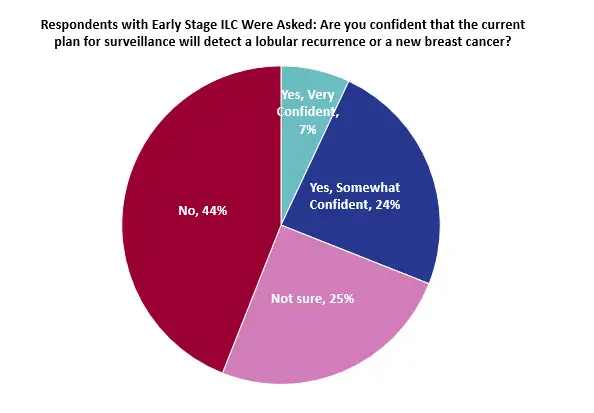
For those who responded “No” to the question of “Are you confident that the current plan for surveillance will detect a recurrence of progression?”we highlighted the following themes.
- Among those with early-stage ILCA, who said they were not confident in the imaging aspect of the surveillance plan, most felt they needed to self-advocate for something more or different from what their surveillance plan called for.
“I know it’s hard to detect and am always fearful that it is still in me somewhere.”
“From my own research, I understand how different this cancer presents itself, and I know that it is more common to have a later recurrence than from ductal. I also don’t think most clinicians understand the difference, and what they should really be looking for.”
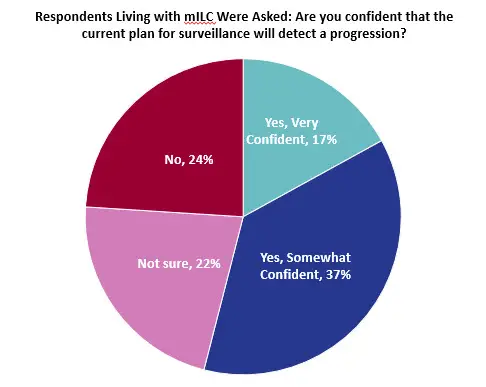
- And for those living with metastatic ILC, mistrust in imaging used in current surveillance plans and the fact that it often did not find the cancer initially or failed to find previous progressions were common themes among those with no confidence.
“I routinely have symptoms of progression before it is visible on MRI or CT scans.”
“It wasn’t picked up for 3 years of imaging prior to diagnosis therefore de novo.”
- Finally, we found that reported high rates of fear of cancer recurrence/progression were correlated with lack of confidence in surveillance plans.
Conclusions
What was clear is that patients need clear, consistent, and ILC-specific surveillance plans and tools so patients feel safer, better supported, and more confident. However, data on the optimal type and frequency of surveillance testing is needed to inform ILC-specific plans. Like many areas of ILC treatment, the area of surveillance needs more research to inform ILC-specific practices. LBCA continues to support ILC specific research, and we will continue until we live in a world in which lobular breast cancer is found early, treated effectively, and eradicated permanently.
Next Steps
There is a wealth of information that remains to be analyzed in the survey data, including much of the descriptive responses. Our plans are to use the information along with data from our past surveys to develop and publish a manuscript that will paint a full picture of the challenges faced by individuals who have had or are living with an ILC diagnosis.
See the poster of these results that we presented at SABCS 25 here.