The 2022 San Antonio Breast Cancer Symposium (SABCS22) included more than 20 research posters focused on lobular breast cancer. Posters at research conferences are tools used to present new information, often the synopsis and key findings of a research study, in a graphic.
Following is a collection of lay summaries of many of the lobular breast cancer-specific posters presented at SABCS22. Most summaries include a link to the poster itself.
A poster by the Lobular Breast Cancer Alliance (LBCA) sharing the results of our survey last spring of individuals living with metastatic invasive lobular carcinoma (ILC) is also included in the summaries.
LBCA thanks members of our Scientific Advisory Board, our Board of Directors, our Patient Advocate Advisory Board and poster authors for creating these summaries.
List of Lay Summaries Contained in This Article
(Summaries follow this listing)
PD4-07 Uncovering molecular heterogeneity of mixed ductal and lobular carcinoma using digital spatial profiling
P2-03-13 Breast Cancer Index (BCI) identifies fewer patients with high risk of late recurrence and high likelihood of benefit from extended endocrine therapy with invasive lobular compared to invasive ductal carcinoma
P2-03-16 Quantifying estrogen and progesterone receptor status in early-stage invasive lobular carcinoma of the breast: associated factors and outcomes in an institutional series
P2-21-01 Decoding Inter- and Intra-Tumor Heterogeneity in Lobular Breast Cancer Using Spatial Transcriptomics and Clustering Analysis
P2-21-07 Exploring spatial correlations in Breast invasive Lobular Carcinoma subtypes using a novel CAF multiplex immunofluorescence panel
P2-21-08 Digital spatial profiling of RNA and protein in the invasive lobular breast cancer microenvironment
P3-05-04 Absence of Lobular Carcinoma in Situ, a Poor Prognostic Marker in Invasive Lobular Carcinoma
P3-05-08 Prevalence and prognosis of ER-loss in advanced invasive lobular carcinoma
P3-05-35 The impact of parity and age of first full term pregnancy on the prevalence and characteristics of invasive lobular carcinoma
P3-05-38 Biology and clinical course of lobular cancer in breast cancer
P3-05-40 Lay summary: Association of body mass index with clinicopathological features and survival in patients with primary invasive lobular breast cancer
P3-08-10 Combining multiomics and histological assessment to identify patient derived xenograft models of invasive lobular carcinoma
P4-01-24: Targeting receptor tyrosine kinases in overcoming tamoxifen resistance and dormancy in invasive lobular cancer
P4-02-04 Serial monitoring of circulating tumor cells and circulating tumor DNA in metastatic lobular breast cancer identifies intra-tumor heterogeneity and precision and immuno-oncology biomarkers of therapeutic importance
P4-02-25 Analysis of prognosis in different subtypes of invasive lobular carcinoma using a National Cancer Database Breast Cancer Registry of Japan
P4-03-11 Population-based survival outcomes of pure vs mixed invasive Lobular Breast Carcinoma in Ontario, Canada
P5-14-01 Transcriptomic insights into lobular breast cancer biology: a retrospective analysis of the MINDACT clinical trial
P6-01-30 PgR levels and Ki67 expression of lobular carcinomas of the breast might indicate OncotypeDX testing to evaluate chemotherapy benefit
P6-05-50 Lobular Breast Cancer Alliance Inc. Survey of Individuals with Metastatic Invasive Lobular Carcinoma
P6-08-09 Self-identified race and Area Deprivation Index in patients with invasive lobular carcinoma of the breast: associations with tumor characteristics and event free survival
Lay Summaries
PD4-07 Uncovering molecular heterogeneity of mixed ductal and lobular carcinoma using digital spatial profiling
{kind=link}
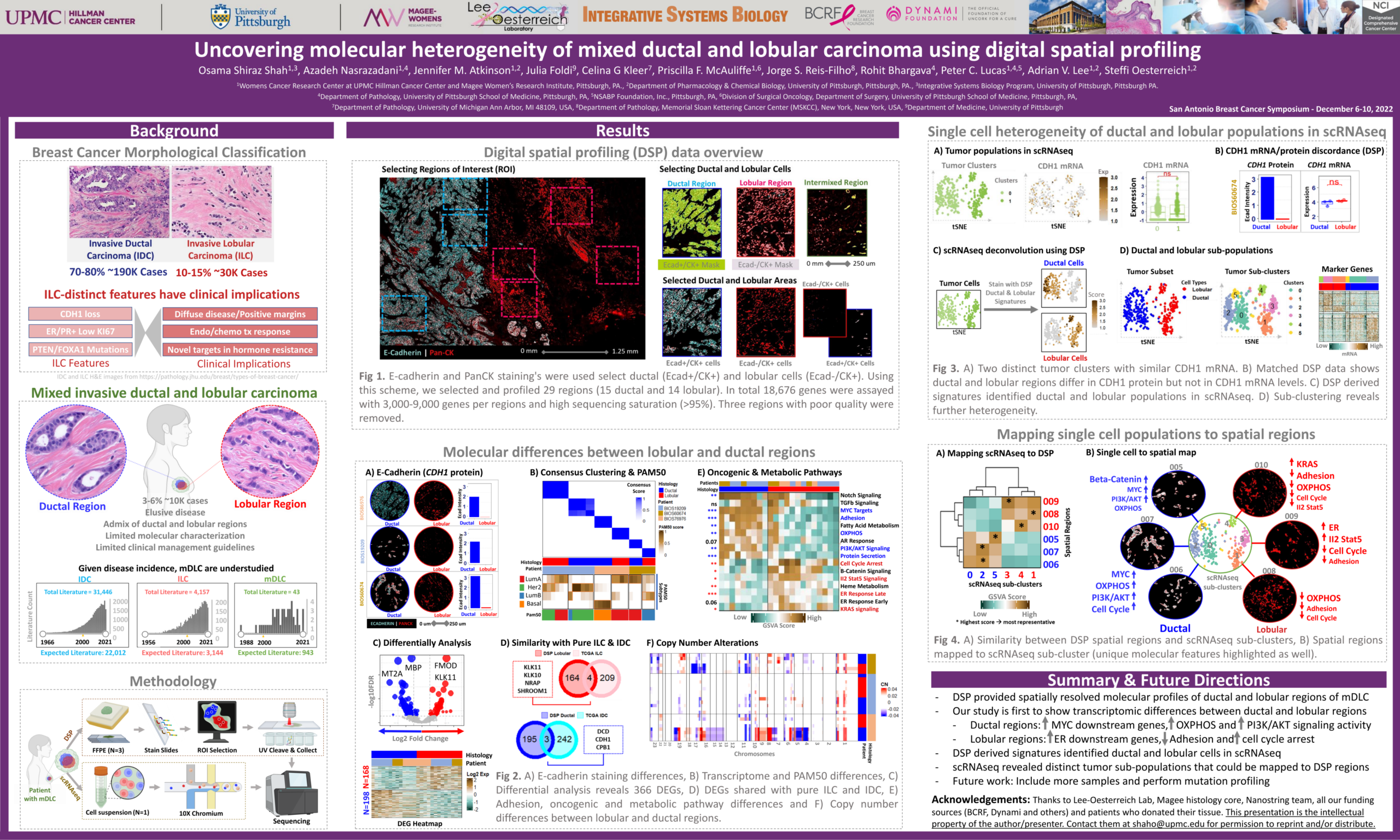
Summary: Approximately 3-6% of all breast cancers contain both histological subtypes, ductal and lobular components. Using advanced technologies, we have studied some mixed tumor cases and have shown that the differences in pathology are reflected in differences in the molecular make-up of the ductal and lobular components.
Study Specifics/Study Goal: Tumor sequencing was performed using advanced technologies, such as digital spatial profiling, which enables viewing of tissue in a way that combines gene expression profiling with immunohistochemistry, to enable better evaluation of cellular interactions, tissue heterogeneity, and pathogenicity, and response to therapy, among other things. This study used this technique to study patients with tumors that were mixed – invasive ductal (IDC) and invasive lobular carcinomas (ILC) to evaluate the molecular profiles of the two subtypes.
Population/Study: Tumor samples from patients with mixed IDC/ILC.
Results: Researchers were able to demonstrate that the spatial profiling signatures identified lobular and ductal tumors, and identified some transcriptomic differences between the two (lobular had increased ER downstream genes, decreased adhesion genes, and increased cell cycle arrest as compared to IDC).
What does this mean for patients?
The findings further delineate transcriptomic differences between ILC and IDC (i.e., differences in molecules in ILC vs. IDC tumors in terms of how they make proteins and perform other functions within the cell). The study is also an introduction of an important new method (digital spatial profiling) to evaluate tumor genetic profiling. In the future this can lead to findings about what might be targeted with specific therapies to best benefit patients with mixed subtypes.
Lay summary prepared by Steffi Oesstereich, PhD, and Tracy Cushing, MD
P2-03-13 Breast Cancer Index (BCI) identifies fewer patients with high risk of late recurrence and high likelihood of benefit from extended endocrine therapy with invasive lobular compared to invasive ductal carcinoma
The goal of this study was to compare Breast Cancer Index (BCI) test results of patients with invasive lobular carcinoma (ILC) as compared with patients with invasive ductal carcinoma (IDC), as these two histologic subtypes have different prognoses and responses to treatment. The BCI is a validated genomic assay that provides the risk of overall (0-10y) and late (5-10y) distant recurrence (DR) and predicts the likelihood of benefit from extended endocrine therapy (EET).
The population used for this study comes from a database of cases submitted for BCI testing in clinical practice, as well as patients with ILC treated in the IDEAL (Investigation on the Duration of Extended Adjuvant Letrozole) trial, that examined the benefit of extended durations of AI therapy.
Within the BCI clinical database, the analysis showed that although patients with ILC had larger tumor sizes, they were considered to be less aggressive than IDC based on clinical and pathological factors. BCI prognostic results were consistent with these findings showing fewer patients with ILC at high risk for late DR compared to IDC. ILC patients within the IDEAL cohort were also found to have lower risk overall. While fewer patients with ILC were predicted to benefit from EET based on BCI (H/I)-High status, they still derived similar absolute benefit compared to the overall cohort, while those classified as BCI (H/I)-Low status derived no benefit from EET. These results are promising regarding the clinical utility of using BCI testing in the future for prognostication and prediction of EET benefit for patients with ILC.
Lay summary by Kai Treuner, PhD
P2-03-16 Quantifying estrogen and progesterone receptor status in early-stage invasive lobular carcinoma of the breast: associated factors and outcomes in an institutional series
{kind=link}
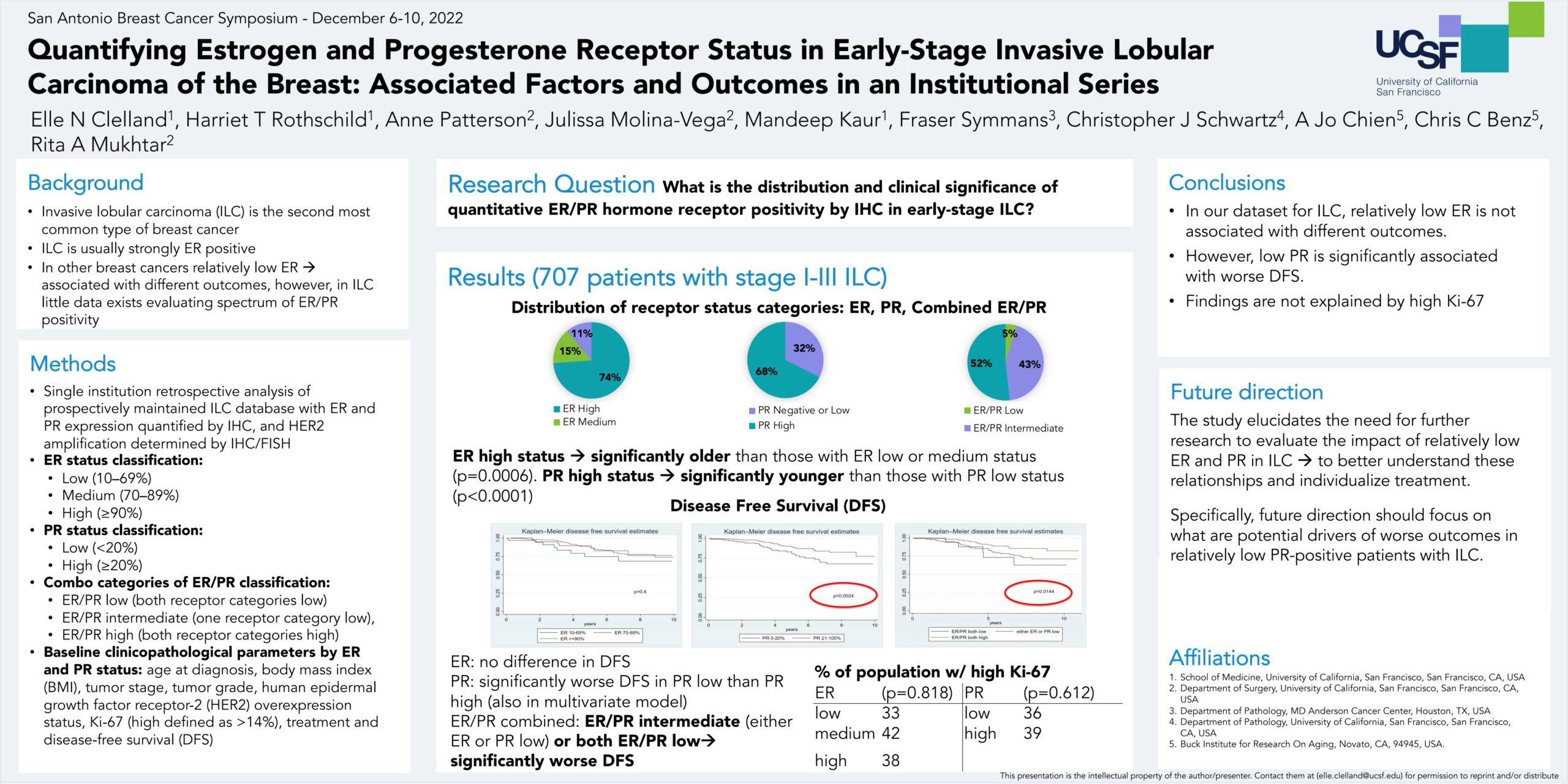
The researchers were interested in understanding the distribution and the clinical significance of positive estrogen receptors (ER) and positive progesterone receptors (PR) in early-stage invasive lobular carcinoma (ILC) tumors. They noted that overall, ILC is typically regarded as strongly ER and PR-receptor positive but there is very little data evaluating the range of hormone receptor positivity in ILC. Using one institution’s prospective ILC database, they looked at the patient characteristics, tumor features, and disease-free survival of patients based on different levels of ER and PR receptor positivity. Levels of hormone receptor positivity were defined according to the amount of estrogen and progesterone receptor staining seen in tumor tissue samples. Based on the percentage of receptor staining observed, ER positive status was defined as low (10–69%), medium (70–89%), or high (≥90%), while PR positive status was defined as either low (<20%) or high (≥20%). “Combo” ER/PR categories were defined as “ER/PR low” (both receptor categories low), “ER/PR intermediate” (one receptor category high or medium), or “ER/PR high” (both receptor categories high).
Overall, patients with either “ER/PR low” or “ER/PR intermediate” receptor status were found to have significantly worse disease-free survival. When PR and ER status were looked at separately, patients with PR low receptor status had significantly worse rates of disease-free survival, whereas among patients having ER low, ER medium, and ER high status there was no statistically significant difference in disease-free survival. Additionally, ER high patients were found to be significantly older, while PR high patients were significantly younger.
The researchers considered whether the worse disease-free survival seen in the PR low cases might correlate with a particular proliferative tumor subtype (called “luminal b”). They tested the association by looking for an association in PR low cases with high ki-67 levels (the cancer-related gene that when found in high levels can indicate a rapid reproduction of cancer cells). There did not appear to be an association. This study highlights the need for further research looking at the range of ER and PR receptor positivity in ILC and at what might be driving the less favorable outcomes that were seen in patients with low PR.
Lay summary provided by Elle Clelland
P2-21-01 Decoding Inter- and Intra-Tumor Heterogeneity in Lobular Breast Cancer Using Spatial Transcriptomics and Clustering Analysis
Recent studies showed that underlying heterogeneity found within the same tumor, referred to as intratumor heterogeneity, (meaning there are distinct tumor cell populations within the same tumor) has an impact on patient outcome.
Our study goal was to obtain more information about tumor heterogeneity and about how genetic differences between cancer cells in the same tumor impact patient outcomes.
Spatial transcriptomics is a technique that allows us to sequence the RNA of a group of cells (i.e., study the entire genetic makeup of the cells) and, subsequently, to map the gene expression on the original histological image (keeping the spatial information). Here, we aimed to better characterize intra- and inter-tumor heterogeneity in invasive lobular carcinoma (ILC) using spatial transcriptomics (ST) together with high-resolution morphological annotation of the relative histological slides (i.e., to use the techniques for gene sequencing and looking at gene expression map along with the original microscopic picture of the tumor to obtain more information about the heterogeneity of the tumor and information about what this means for patient outcome).
Study Population/Methods: Spatial transcriptomics was performed on frozen tumor samples obtained from 43 patients with estrogen receptor-positive, HER2-negative ILC, of which 9 developed disease relapses. 32 samples from patients’ tumors were analyzed. The researchers aimed to describe the intra- and inter-tumor heterogeneity by identifying common or specific characteristics across different tumors. Intra-tumor heterogeneity was highlighted by the presence of different tumor clusters inside the same sample. A tumor cluster enriched in proliferation-related pathways was found to be more present in samples with higher tumor grade. Tumor clusters enriched in inflammation-related pathways were found to be more present in samples with higher tumor stages. A higher spatial disorganization of tumor cells (so a greater number of contacts between cancer cells and other microenvironment cells) was observed in samples coming from patients who experienced disease relapse. This indicated that tumors with more genetic differences were found to have higher grades and tumor stages.
What this means for patients is that the presence of shared biological processes across ILCs, as well as the role of heterogeneity and specific pathways may be associated with the risk of recurrence.
The researchers noted that further research should be done to further characterize the processes within the tumors and identify therapeutic biomarkers and tumor features which may not be evident from common sequencing analyses. They noted the need for further validation of their findings.
Lay summary by Matteo Serra, MS, and Theresa Langdon, MD
P2-21-07 Exploring spatial correlations in Breast invasive Lobular Carcinoma subtypes using a novel CAF multiplex immunofluorescence panel
{kind=link}
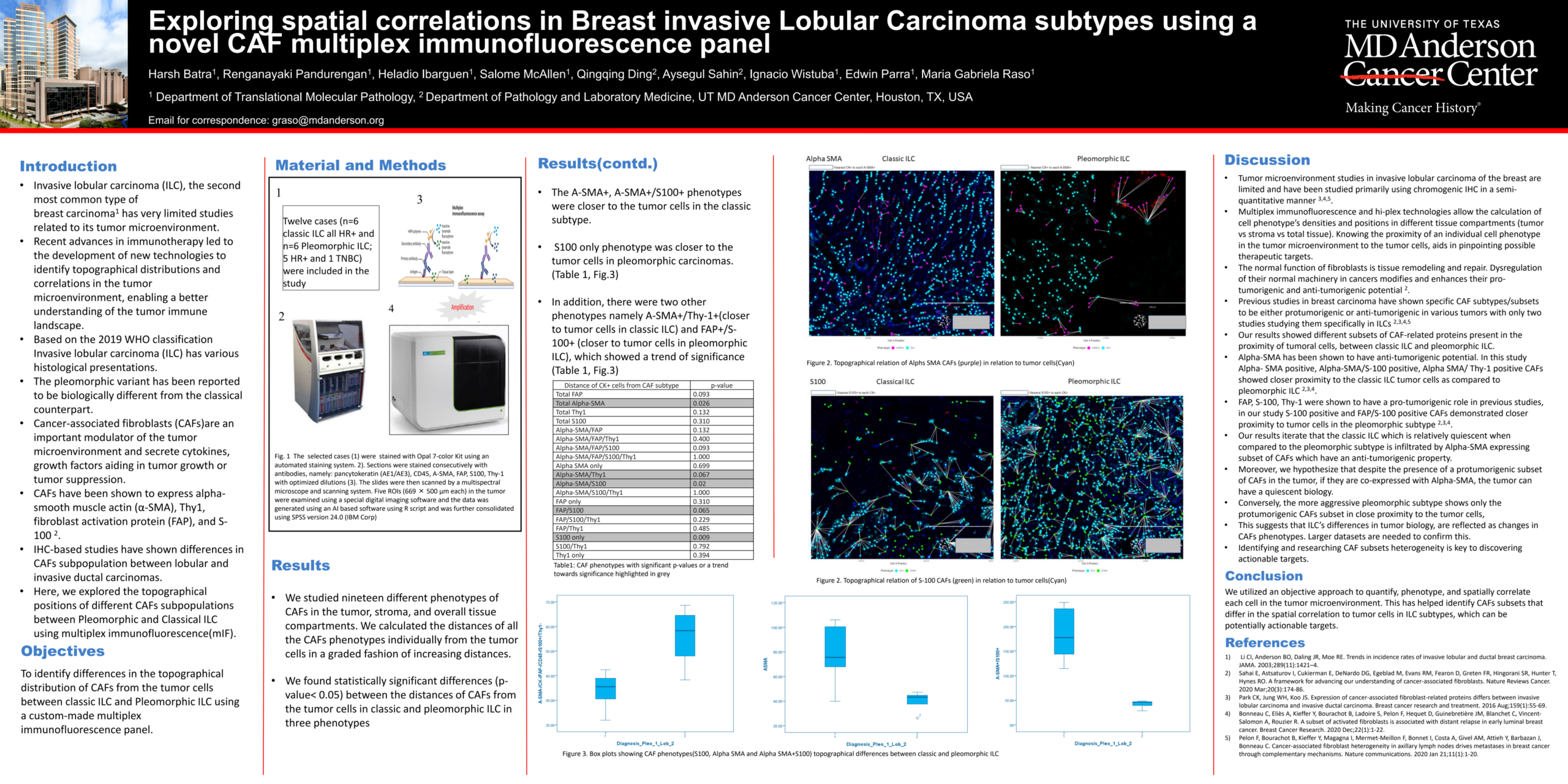
Recent advances in immunotherapy led to the development of innovative technologies to identify topographical distributions and correlations in the tumor microenvironment, enabling a better understanding of the tumor immune landscape.
Invasive lobular carcinoma of the breast (ILC) has various histological presentations. The pleomorphic variant has been reported to be biologically different from the classical counterpart. Cancer-associated fibroblasts (CAFs) are central players in the microenvironment of solid tumors, affecting cancer progression and metastasis. CAFs have diverse phenotypes (i.e., the observable characteristics related to the expression of genes), origins and functions and consist of distinct subpopulations. CAFs secrete cytokines (a type of protein) and tumor growth factors aiding in tumor development and invasiveness. Fibroblast dysregulation in cancer enhances their pro-tumorigenic (causing tumors) and anti-tumorigenic potential.
The main objective of this study was to explore different CAF sub populations between Classical and Pleomorphic ILC variants using a technique called Multiplex Immunofluorescence, which is a hi-plex (enables screening of sequencing many samples in one flow-cell lane) technology that allows the visualization of multiple bio markers in one tissue section. Using a small ILC cohort, this technology and using spatial analysis, we were able to determine differences among them.
We found that Pleomorphic ILC is strongly associated with pro tumorigenic CAFs subpopulations while Classic ILC shows a myofibroblast profile (i.e., with many myofibroblasts) that can be effective therapeutic targets.
In conclusion, we utilized an objective approach to quantify, phenotype and spatially correlate each cell in the tumor microenvironment. This has helped identify CAFs subsets that differ in the spatial correlation to tumor cells in ILC subtypes, which can be potential actionable targets for therapies. Further validation of these findings is currently ongoing in a larger cohort.
Lay summary by Maria G. Raso, MD
P2-21-08 Digital spatial profiling of RNA and protein in the invasive lobular breast cancer microenvironment
Invasive lobular breast cancer (ILC) is an understudied subtype of breast cancer with late recurrence, metastasis to distant sites, such as the peritoneum, and poor long-term outcome. The glucocorticoid receptor (GR) is the receptor in a cell for the body’s stress hormone. Our preliminary data suggested there might be a more favorable patient outlook in the ILC when tumors express higher levels of GR.
Tumor cells don’t exist alone but are surrounded by, and interact with, other cells and proteins that form what we call the stroma or tumor microenvironment (TME). ILC is different to invasive ductal carcinoma in that tumor cells grow as single files due to lack of E-cadherin, a protein that is important for cell-to-cell interactions. Because of these differences we expect the TME to be quite unique in ILC compared to other breast cancer subtypes.
We selected primary ILC tumors with a wide variation in GR expression, ranging from completely negative to strongly positive. Our goal was to gain insight into how GR presence or absence in ILC might impact the genes and proteins expressed in the tumor cells or the surrounding stromal cells. We used the state-of-the-art nanoString GeoMx® platform that enabled us to look at the gene and protein expression for the tumor cells and the surrounding cells separately, or “spatially”.
We first performed spatial gene and protein expression for 12 primary ILC tumors, some of which were strongly positive for GR, some GR-negative and 2 “mixed” tumors with GR-positive and GR-negative regions. We compared the genes and proteins in the GR-positive versus GR-negative cancer cells and stromal cells separately and observed intriguing differences.
Interpretation of the gene expression in the stromal cells revealed striking differences between the abundance of certain subsets of immune cells and other cell types surrounding the GR-positive versus the GR-negative cancer cells. Interestingly, evidence supported the presence of significantly higher numbers of macrophages and suppressive myeloid cells (cell types helpful in killing cancer cells) surrounding GR-positive ILC tumor cells. The abundance of other immune cells (B- and T-cell subsets) as well as endothelial cells and fibroblasts was also notably different. Analysis of RNA and proteins supported an immune-suppressive tumor microenvironment promoted by GR. We also observed suppression of certain immune checkpoint proteins in ILC with high GR expression.
We are currently expanding our study to include additional GR-positive and GR-negative ILC tumors. Thus, we will generate comprehensive molecular profiles of ILC tumors and their surrounding cells to acquire a deeper understanding of how GR expression/activation influences the crosstalk between ILC tumor cell and the stroma. We anticipate that these data will provide clues as to how GR activation affects the growth and invasive properties of ILC through modification of their surrounding cells. We hope to expose vulnerabilities in ILC that can be targeted therapeutically to improve patient outcomes.
Lay summary by Lynda Bennett, PhD
P3-05-04 Absence of Lobular Carcinoma in Situ, a Poor Prognostic Marker in Invasive Lobular Carcinoma
{kind=link}
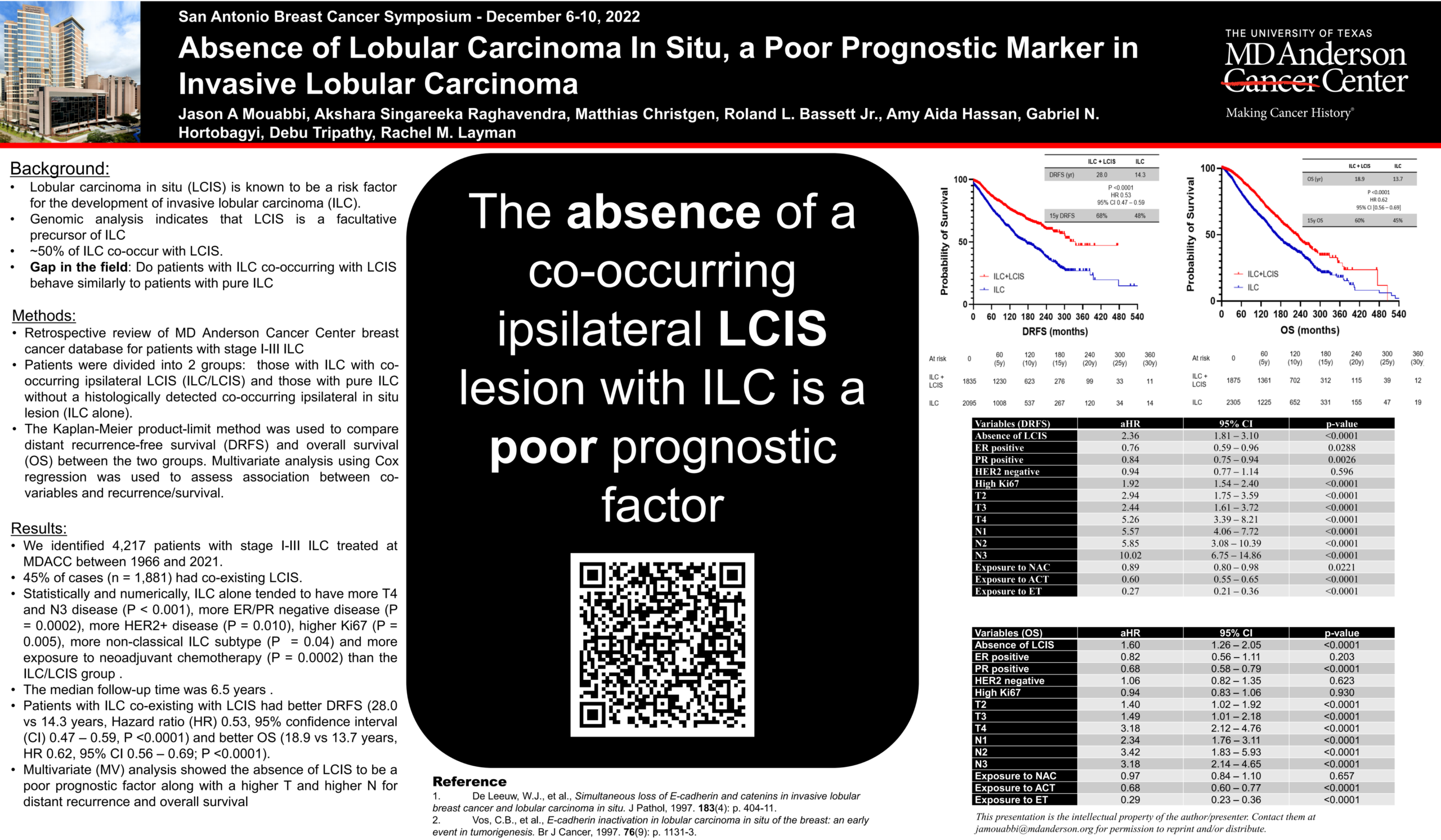
Study Goal: To evaluate whether Invasive lobular carcinoma (ILC) tumors with concurrent lobular carcinoma in situ (LCIS) pathology behave differently than ILC without LCIS.
Population/Study: Retrospective review of MD Anderson breast cancer database of the records from patients with stage 1-3 ILC.
The analysis:
- Looked at the information on patients in two groups (those with both ILC+LCIS, and those with ILC alone)
- Compared distant recurrence-free survival and overall survival between the two groups
- 4,217 cases in the database were identified
- Median follow up time was 6.5 years
Results
- 45% (n=1881) had co-existing LCIS
- Patients with ILC alone had more lymph node involvement, ER/PR negative disease, Her2+ disease, higher Ki-67%, and more non-classical ILC subtypes
- Patients with both LCIS + ILC tumors had better rates of disease free (no recurrence) survival (28 vs 14 years) and better overall survival (18 vs 13 years)
What does this mean for patients?
The analysis suggests that the absence of LCIS may be a poor prognostic factor, along with high T and N stages for distant recurrence and overall survival. The scientists noted that further analysis of these findings is being conducted and further study warranted.
Lay summary by Tracy Cushing, MD
P3-05-08 Prevalence and prognosis of ER-loss in advanced invasive lobular carcinoma
Loss of estrogen receptor expression (ER-loss) is known to occur in about 20% of breast cancers at the time of recurrence, and results in worse outcomes for the affected patients as these cancers no longer respond to anti-estrogenic endocrine therapy. Invasive lobular carcinomas (ILC) are characterized by high levels of hormone receptor expression and are less responsive to chemotherapy compared with other types of breast cancer. The impact of ER-loss in ILC is unknown.
Patients with advanced breast cancer often have tumor tissue sent for genomic testing (analysis of the tissue’s genetic composition). CARIS, Inc. is a company which performed such testing and has created a searchable database combining their genomic data with clinical information obtained from insurance claims. The investigators searched this database to identify breast cancers with ER-loss, which were defined as cancers which tested negative for estrogen receptor after prior treatment with endocrine therapy. ER-loss occurred in 11.4% of ILC tumors and in 19.6% of invasive ductal carcinomas (IDC). Overall survival was significantly worse for patients with ILC who had experienced ER-loss compared to patients with ILC without ER-loss. Overall survival was also significantly worse for patients with ILC and ER-loss compared to patients with IDC and ER-loss.
These findings suggest that ER-loss occurs in a subset of patients with ILC and results in poor outcomes. The current standard treatment for breast cancers which have lost estrogen receptor expression is chemotherapy, and it is known that ILC are less responsive to standard chemotherapy than other types of breast cancer. This might explain why patients with ILC and ER-loss had worse survival in this analysis compared to patients with IDC and ER-loss. Newer treatments are needed for patients with ILC who lose estrogen receptor expression at the time of recurrence.
Lay summary by Whitney Hensing, MD
P3-05-35 The impact of parity and age of first full term pregnancy on the prevalence and characteristics of invasive lobular carcinoma
We analyzed the data of patients who were diagnosed with hormone sensitive breast cancer located only in the breast and possibly axillary lymph nodes between 2000 and 2020 in the University Hospitals of Leuven, Belgium. We wanted to see if the number of pregnancies these patients had had and the age at which they had their first pregnancy impacted the chances of having a lobular subtype of breast cancer (ILC). Furthermore, we wanted to see specifically in the patients with ILC, if the number of pregnancies and the age at which they had their first pregnancy impacted the patient (e.g. age at diagnosis, BMI) and tumor characteristics (e.g. tumor grade, size, nodal involvement, expression of the progesterone receptor).
It was found that a higher number of pregnancies seems to be associated with a higher chance of a tumor being lobular when diagnosed with hormone sensitive breast cancer. If women had a higher age at their first pregnancy and they were diagnosed between the age of 41-50, they also had a higher chance of being diagnosed with ILC. The number of pregnancies did not seem to affect the patient and tumor characteristics of ILC.
Acknowledgements: KVB is funded by the KU Leuven Fund Nadine de Beauffort and a Conquer Cancer – Lobular Breast Cancer Alliance Young Investigator Award for Invasive Lobular Carcinoma Research, supported by Lobular Breast Cancer Alliance. Any opinions, findings, and conclusions expressed in this material are those of the author(s) and do not necessarily reflect those of the American Society of Clinical Oncology® or Conquer Cancer®, or Lobular Breast Cancer Alliance.
Lay summary by Karen Van Baelen, MD
P3-05-38 Biology and clinical course of lobular cancer in breast cancer
{kind=link}
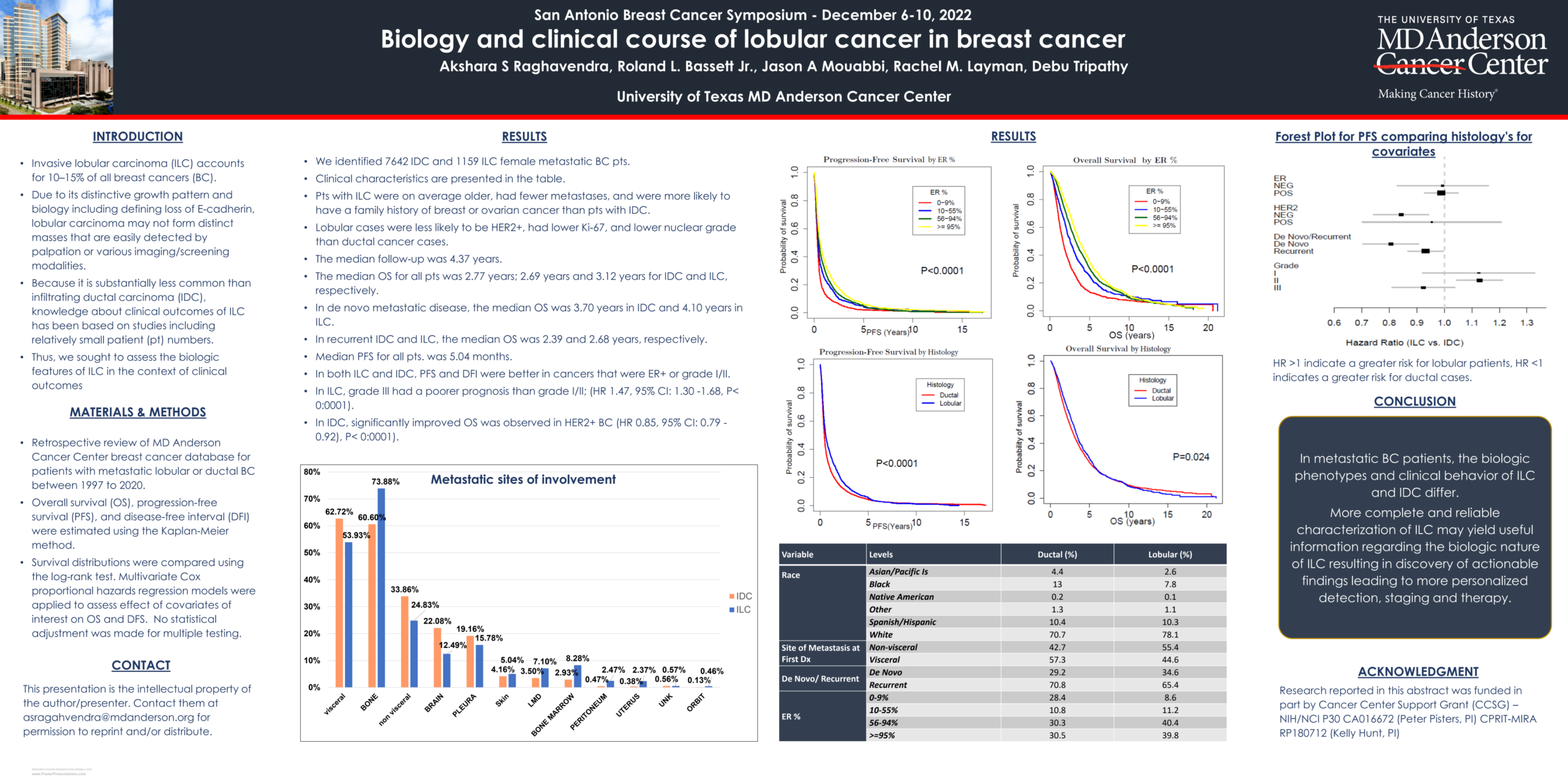
Study Goal: To assess the biologic features of invasive lobular carcinoma (ILC) in the context of clinical outcomes.
Population/Study: Retrospective review of MD Anderson breast cancer database of patients with stage 4 ILC and IDC.
The Analysis:
- Patient data was grouped by those with ILC vs IDC
- 7,642 cases of patients with IDC and 1159 cases of patients with ILC were identified in the database
- Comparisons were made between the two groups with respect to metastatic sites of involvement, distant recurrence-free survival, and overall survival
- Median follow up time was 4.37 years
Results:
- In metastatic breast cancer patients, the biologic phenotypes (the observable characteristics) and clinical behavior of the ILC and IDC tumors differ.
- ILC and IDC metastasized differently at first dx: 42.7% of the metastasis in patients with IDC were to non-visceral sites (i.e., not relating to internal organs) compared to patients with ILC who had metastases to non-visceral sites (55.4%). In contrast, metastases to visceral sites (pertaining to internal organs) among patients with IDC was found in 57.3% of cases compared to ILC at 44.6%.
- ILC patients had better progression free survival compared to IDC up until 5+ years. In contrast, IDC had better overall survival after 10 years.
What does this mean for patients?
- This type of research provides useful information regarding the differences between the biological nature of ILC and IDC.
- Such data will ultimately lead to more personalized detection, staging, and therapy for ILC patients.
Lay Summary by Gitte H. Joergensen, PhD
P3-05-40 Association of body mass index with clinicopathological features and survival in patients with primary invasive lobular breast cancer
{kind=link}
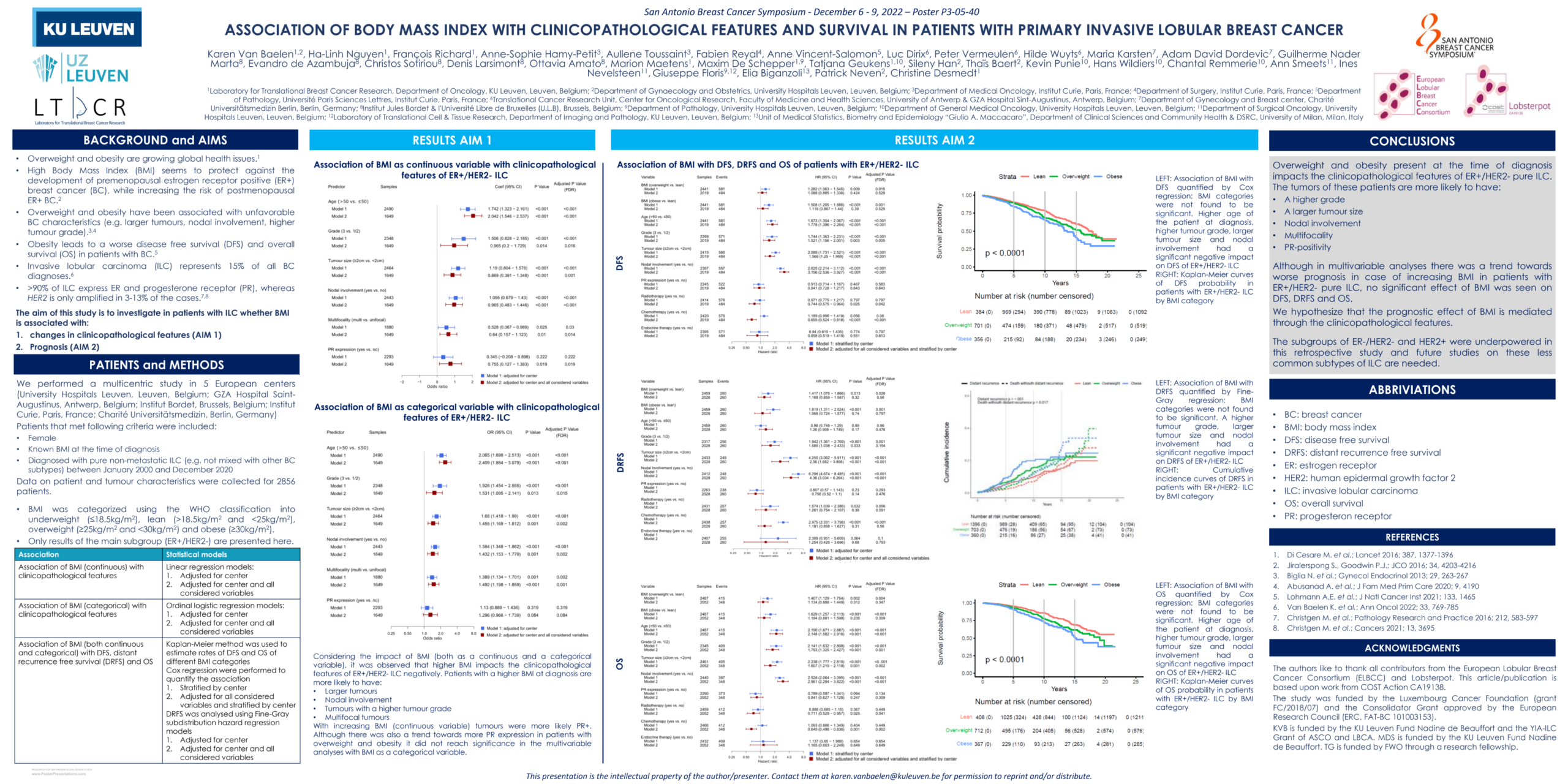
We have collected data in 5 different European centers on body mass index (BMI) and patient (e.g. age) and tumor characteristics (e.g. size, tumor grade, involvement of lymph nodes) of patients that were diagnosed with invasive lobular breast cancer (ILC) between the year 2000 and 2020, who did not have any signs of metastases at the time of diagnosis. The 2 aims of this study were to see if BMI is associated with 1) different patient and tumor characteristics and 2) different survival outcomes in patients with ILC.
We found worse tumor characteristics, like higher tumor grade, larger size, nodal involvement were all associated with a higher BMI at diagnosis. When looking only at BMI and survival outcomes, we saw more recurrences and more deaths with higher BMI. When considering also the impact of other patient and tumor characteristics, there was no longer evidence that BMI impacts the survival outcomes. However, tumor grade, size, nodal involvement were all associated with survival outcomes.
What does this mean for patients: A higher, BMI might indirectly impact the chances to form metastases and the survival of patients with ILC.
Lay summary by Karen Van Baelen, MD
P3-08-10 Combining multiomics and histological assessment to identify patient derived xenograft models of invasive lobular carcinoma
{kind=link}
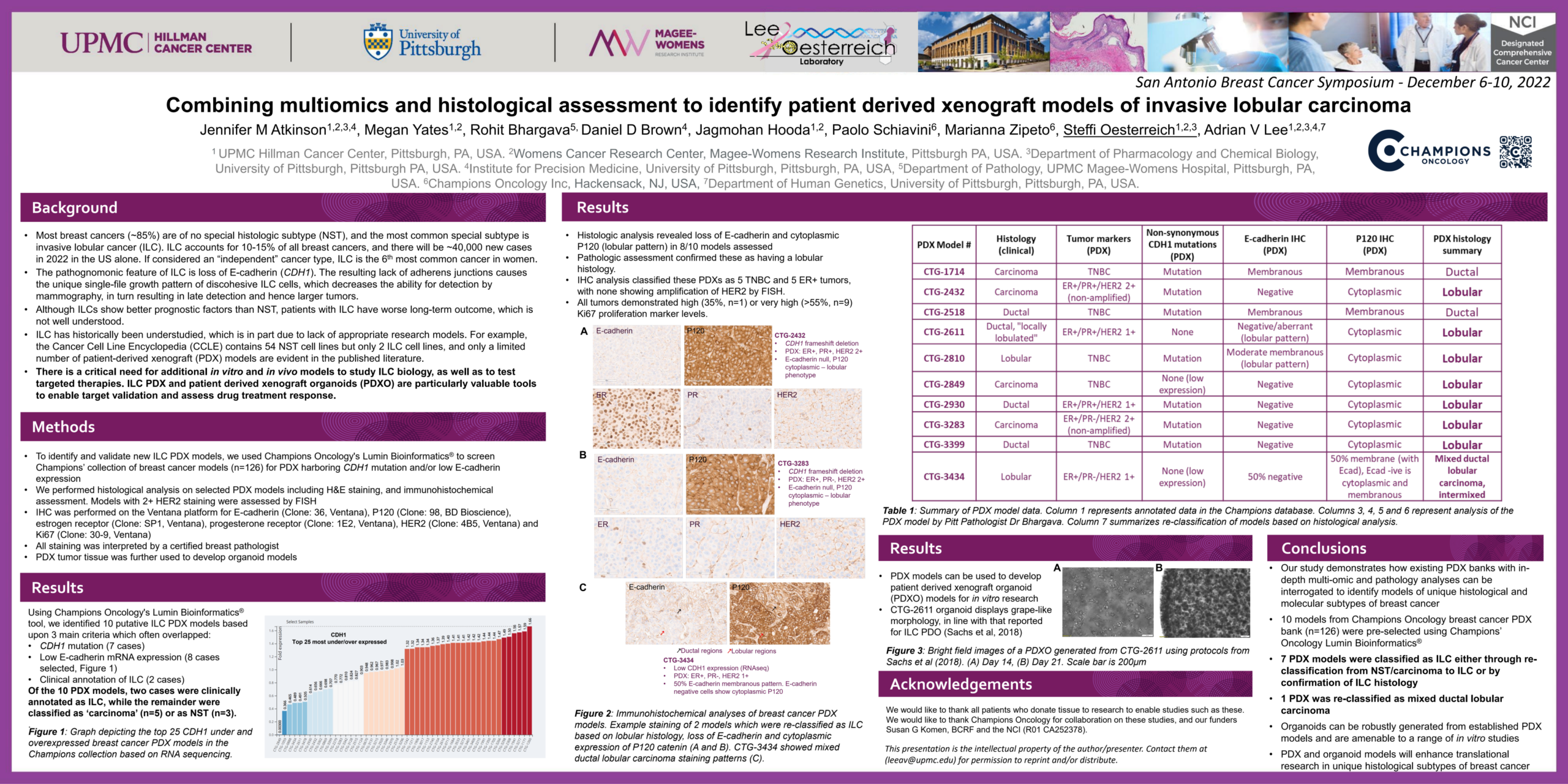
Summary: Research of invasive lobular carcinoma (ILC) has been limited in part due to limited models faithfully representing the disease. In this project, we collaborated with Champions Oncology to identify new mouse models of ILC. Using genomics approaches, and staining of tumors grown in mice, we have identified and validated additional ILC models that will be helpful for future studies of ILC.
Study Goal: To develop patient-derived xenograft models of ILC and subsequently organoid models, to improve researchers’ abilities to conduct in vitro and in vivo studies on ILC biology and response to therapy. Currently such models are few in comparison to research models available for the study of invasive ductal carcinomas or breast cancers of no specific type.
Population/Study: 10 models were assessed. 8/10 had loss of E-cadherin, 5 were triple negative breast cancer (TNBC), and 5 were estrogen receptor positive (ER+). All models showed high levels of ki67.
Results: Xenograft models were successfully used to develop organoid models from established xenograft lines.
What does this mean for patients? The identification of new ILC research models gives researchers more options for conducting in vivo research (i.e., taking place in a living organism) on ILC.
Lay summary by Steffi Oesterreich, PhD, and Tracy Cushing, MD
P4-01-24 Targeting receptor tyrosine kinases in overcoming tamoxifen resistance and dormancy in invasive lobular cancer
Patients with invasive lobular cancers (ILC) face poor long-term disease-free and overall survival. ILC accounts for ~15% of all breast cancers and are usually estrogen receptor (ER), progesterone receptor (PR) positive, and HER2 negative with a low mitotic index (measure of how quickly cells are dividing), leading to slow growth and late recurrence. The hurdles in managing ILC are: a) inherent resistance to endocrine therapy, and b) the possibility that early disseminated tumor cells (DTCs) continue to exist and remain dormant and that this leads to late recurrences and worse overall outcomes. Loss of E-cadherin is the hallmark of ILC, which results in the unique morphology and unusual metastatic spread to serosa (i.e., the outer linings for organs and body cavities) including ovaries, gut, and peritoneum. Despite these unique features, ILC is frequently lumped with ER/PR-positive invasive ductal cancers (IDC); consequently, ILC screening, treatment, and follow-up strategies are primarily based on data from IDC. Hence, there is an unmet need to address the unique features of ILC. Our overarching goal is to improve the long-term outcomes in patients by identifying effective agents that are effective in ILC and will inhibit DTCs, induction of dormancy, and establishment of overt metastases.
Resistance to endocrine therapy in breast cancer is closely associated with the upregulation of receptor tyrosine kinases (RTKs). However, studies targeting single tyrosine kinases, e.g. FGFR, have not been successful. Thus, we have chosen to target multiple RTKs alongside ERα to improve outcomes for ILC patients.
Study goal: We hypothesized that the FDA approved RTK inhibitor Lenvatinib will overcome the characteristics that cause ILC to become endocrine resistant. We posited it would do so by increasing cell death and reducing DTCs, and curtailing induction of dormancy. We anticipate that understanding the DTCs in the context of ILC will equip us to address late recurrences in ILC patients.
Results: We have tested the efficacy of lenvatinib using ILC cell lines. Lenvatinib inhibits multiple growth pathways such as, VEGFR1-3, FGFR1-4, PDGFRα, KIT, and RET. Our preliminary data show that in tamoxifen-resistant (TAMR) ILC cells, the Lenvatinib and tamoxifen combination markedly reduced cell viability compared to tamoxifen alone. Dr. Reategui’s lab has developed novel 2D/3D cell culture in vitro (in a petri dish or by other means outside of an organism) models to study dormancy in ILC cells, as well as the impact of drug treatment. Our data demonstrate our ability to recapitulate and differentiate the morphologies observed in breast tissue for IDC and ILC. They have engineered a microfluidic method to isolate viable circulating tumor cells (CTCs) from blood at high efficiencies and low contamination rates.
Our goal is to:
- Find novel therapies to improve long-term cure rates and
- Characterize the biological relevance of tissue engineering technologies to address a critical question in a cancer that affects ~ 43,000 women in US annually.
Lay summary by Bhuvan Ramaswamy, MD
P4-02-04 Serial monitoring of circulating tumor cells and circulating tumor DNA in metastatic lobular breast cancer identifies intra-tumor heterogeneity and precision and immuno-oncology biomarkers of therapeutic importance
The intention of this study was to determine whether analysis or “sequencing” of circulating tumor cells can contribute more and complementary information about an individual’s tumor and identify potential therapeutic targets that may have been missed when just studying a patient’s tissue biopsy or CtDNA liquid biopsies alone.
Background
Cancer biomarkers, commonly detected from a tumor tissue biopsy, help doctors determine its aggressiveness and guide therapy decisions. However, tissue biopsies are usually limited to a one-time procedure which can be invasive, prone to complications and high-cost. In metastatic patients it is usually performed once early on, thus failing to reveal the states into which the tumor later evolves. Likewise, not all tumor cells in a patient, or even in a tumor mass, are identical at any time. The tumor is often heterogeneous, i.e. it is composed of various clonal cell populations* with different characteristics. One clone or another may become dominant or recede based on the pressures of therapy, the immune system, metabolic constraints etc. A tissue biopsy, which samples a small region, may miss the full picture of that tumor clonal makeup.
Liquid biopsies refer to the isolation of small amounts of tumor material that is released and ends up in a body fluid such as blood. They offer the opportunity to obtain cancer molecular information that represents the entire disease, much more easily, and repeatedly, compared to tissue biopsies. Liquid biopsy in the form of circulating tumor DNA (ctDNA, cell-free DNA derived from dying tumor cells) provides an opportunity to detect and track DNA biomarkers over time. Limitations of using CtDNA include the fact that there is often only a low amount of tumor derived DNA in blood and it only provides DNA-derived information. Similarly, ctDNA, even when present in high enough quantity, can only provide a composite picture of all tumor DNA mutations and not information on the clonal makeup of the tumor at the level of individual clones*.
Circulating tumor cells (CTCs), another form of liquid biopsy sample, which are whole cells breaking off of a tumor mass, can be isolated from blood and offer a unique opportunity to combine the high information content of tissue biopsies with the versatility and non-invasiveness of ctDNA. Using a simple blood draw, we have enabled CTC counting, purification at the individual cell level and analysis of their important proteins and DNA mutations present. Single-cell analysis of CTCs, pioneered by our group, enables us to define the precise clonal architecture as we can group individual cells into the clones they belong to, as opposed to getting a composite picture or everything in one. Although these cells are rare in blood, especially in earlier phases of the disease and certain cancer types, we and others have shown that lobular breast cancer is an especially high CTC-producing cancer type particularly suited to CTC analysis.
Methods and Results
We analyzed tissue, ctDNA and 113 single CTCs from 15 metastatic lobular breast cancer patients with abundant tumor cells in circulation.
We found that 60% of patients harbored DNA defects in their tumor for which targetable, precision treatments exist. Interestingly, a third of them harbored targetable DNA alterations not detected in all three sample types (tissue, ctDNA and CTC). These included 3 actionable mutations found in CTC and ctDNA only, 1 in tissue and ctDNA only, and 1 in ctDNA only. However, 2 of those ctDNA mutations were identified near or below the “limit of detection” i.e., as low-confidence, or “soft” calls but were included with the help of a priori knowledge of their presence from tissue or CTCs. Further, 1 patient with plentiful CTCs had no detectable ctDNA, and one patient’s tissue biopsy was inadequate for sequencing while both liquid biopsy samples were abundant. 87% of patients harbored heterogeneous tumors in their CTC that were not detected or ambiguous in their tissue biopsy or ctDNA. A deep dive into a patient’s 2 tissue biopsies, 5 ctDNA samples, and 30 individual CTC combined to reveal in unprecedented detail such tumor heterogeneity and evolution in response to endocrine and immunotherapy selective pressures. CTC provided an additional level of detail of the full heterogeneous picture not appreciable in the other two sample types.
Developing an innovative technique, we also enabled detection of single-cell CTC Tumor Mutation Burden (TMB) and Microsatellite Instability (MSI), two important biomarkers that predict immunotherapy response. Lobular breast cancer has been shown to have a higher TMB than ductal cancer, making some patients eligible for immunotherapy. Yet, monitoring of such immunotherapy biomarkers beyond the initial detection is not currently done. While cancer biomarker detection will probably always include analysis of the initial tissue biopsy, work has shown that the further away in time a tissue and a ctDNA analysis of a patient are separated, the more discordant they are. This suggests that the tumor evolves, and monitoring by liquid biopsy becomes essential. This technique is being developed for use in the clinic to aid monitoring tumor evolution.
CTC TMB values in our patients were concordant with those detected in tissue. We also made a novel observation, (i.e. a concept not yet reported in literature): we detected heterogeneity and evolution of these immunotherapy biomarkers in CTC over time. In one patient, two individual TMB-low CTC clones combined to yield a TMB-high composite value in ctDNA. The latter would erroneously make eligible for immunotherapy a patient that would not benefit. In another patient, an original TMB-low clone became dominant in CTC after the treatment with chemo- and immunotherapy resulted in clearance from circulation of the other, TMB-high CTC clone. Intriguingly, after interruption of this treatment, we isolated CTC that belonged to the TMB-high clone and potentially was still amenable to immunotherapy. If confirmed in other patients, this may be a paradigm-shifting observation that may support future reintroduction of immunotherapy to patients who have originally become resistant to it. Current treatment guidelines consider such patients ineligible for future immunotherapy on account of having once developed resistance, yet our data show this may not always be the case.
Conclusions and Next Steps
Given the propensity of lobular breast cancer to have a higher tumor mutation burden and thus be amenable to immunotherapy, these findings have potential implications for predicting response, allowing monitoring, and enabling early detection of resistance to immune checkpoint inhibitors. Overall, these data support the continued investigation of CTC for clinically important biomarker detection and monitoring to extend survival and eventually eradicate deaths from lobular breast cancer.
* Cells divide by mitosis and generally produce two genetically identical, or clonal daughter cells, although occasional DNA mutations may happen. Cells in a person’s body are usually clonal (as they arose from a single cell). In cancer, an initial normal cell has transformed by gaining one or more DNA errors/mutations/alterations. This makes it grow, divide and proliferate at an increased rate. As this cell gives rise to other cells by copying DNA and passing on those initial mutations in successive generations, one cell, in addition to the original (truncal) mutations, will gain a new mutation. That cell and its progeny, not the rest of the cells, will carry that additional mutation together with the initial ones (forming a branch). The different clones or branches may be in cooperation or competition as the tumor evolves. The presence of many such branches makes curing cancer difficult. Treatments we use may be effective on one or more of such branches, but one or other branches may be resistant. They grow out and become dominant, leading to regrowth of cancer. That said, identification of variants within a population of cancer cells, particularly over time as the cells evolve, can inform the prognosis and treatment of the disease. The authors acknowledge Dynami Foundation for the significant support they provided for this research.
Lay summary by Andi Cani, PhD, and Laurie Hutcheson, MS
P4-02-25 Analysis of prognosis in different subtypes of invasive lobular carcinoma using a National Cancer Database Breast Cancer Registry of Japan
Invasive lobular carcinoma (ILC) is more likely to be hormone receptor (HR) positive, and several studies have reported that the prognosis of ILC was better than IDC. However, ILC also has different prognoses depending on the subtype as compared to invasive ductal carcinomas (IDC), and it may be that the better prognosis for ILC might depend on high hormone receptor positivity. Additionally, there are many reports that chemotherapy (CT) does not improve the prognosis of ILC due to the high positivity of HR.
Study Goal: To compare overall survival between of IDC and ILC; to compare the overall survival between the luminal sub-types of IDC and ILC; and to assess the benefit of chemotherapy in ILC. Luminal sub-types of IDC and ILC are estrogen receptor-positive, progesterone receptor-positive and HER2-negative.
Study analysis was conducted using the Breast Cancer Registry (BCR) run on the National Cancer Database (NCD) in Japan.
Study population:
- 5,633 patients with ILC and 5,633 patients with IDC
- 95 patients with luminal IDC and 95 patients with luminal ILC with tumors between 2-5 cm and no axillary lymph node involvement (T2N0)
- 83 patients with luminal IDC and 83 patients with luminal ILC with tumors less than 5cm and in whom there has been involvement of 1 -3 axillary lymph nodes (T1-2N1)
Results
- Overall, the 10 year disease free survival and overall survival were worse in those with ILC as compared to those with IDC. Among the luminal sub-types of IDC and ILC, luminal ILC had poorer disease free survival and over all survival than IDC. Patients with T1-2N1 luminal ILC who received chemotherapy had a better prognosis than patients with T1-2N1 luminal ILC who did not receive chemotherapy. Patients with pT2N0 luminal ILC showed no benefit from chemotherapy.
What does this mean for patients? The findings suggest that patients with ILC have an overall poorer prognosis than those with IDC. The study suggested that treatment of luminal ILC needs to be differentiated from that for luminal IDC. It also suggested that patients with luminal ILC whose cancer has spread to their lymph nodes may benefit from chemotherapy.
Lay summary by Yayoi Adachi, PhD, and Theresa Langdon, MD
P4-03-11 Population-based survival outcomes of pure vs mixed invasive Lobular Breast Carcinoma in Ontario, Canada
{kind=link}
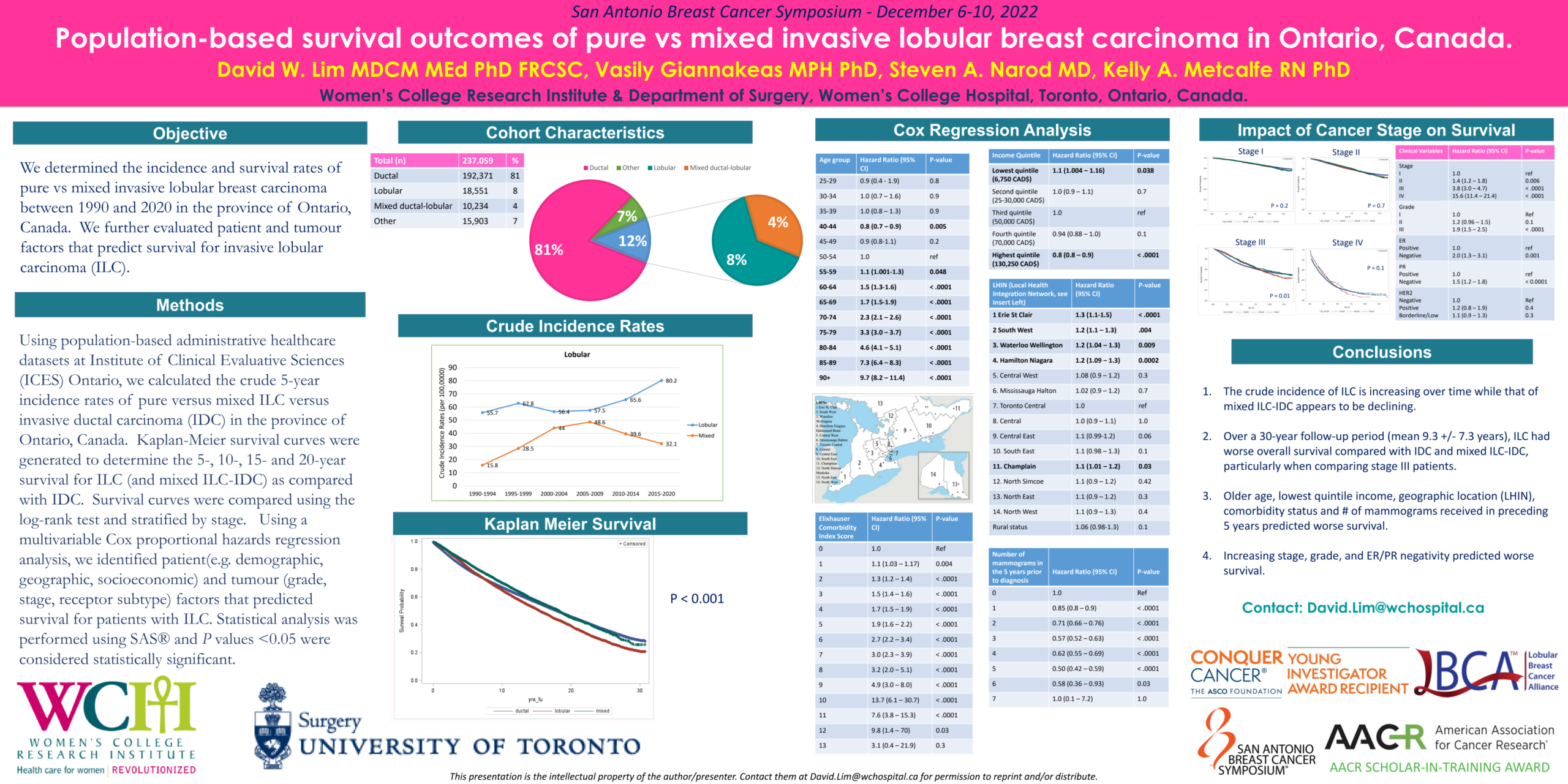
Reasons for the study: Our study had several research questions. First, we wanted to determine contemporary incidence rates of lobular breast cancer and mixed ductal-lobular breast cancer in the province of Ontario, Canada over a 30-year period. Second, we wanted to determine if there was a difference in survival between ductal, lobular and mixed ductal-lobular breast cancer over the same time period. Lastly, we were interested to identify patient and tumor characteristics that predicted worse or better survival in women with lobular breast cancer.
Methods: We used publicly-available administrative datasets that are collected at ICES Ontario, such as the Ontario Cancer Registry, to identify all women who had a diagnosis of breast cancer in the last 30 years. We were able to then calculate raw incidence rates and survival. We used a statistical method called regression analysis to identify patient and tumor characteristics that predicted better or worse survival in women with lobular breast cancer.
Findings:
- The raw incidence of pure lobular breast cancer increased from 55.7 per 100,000 in 1990 to 80.2 per 100,000 in 2020 while that of mixed ductal-lobular breast cancer peaked in the mid-2000s at 48.6 per 100,000 and declined to 32.1 per 100,000 in 2020.
- The survival of women with mixed ductal-lobular breast cancer was similar to women with pure ductal breast cancer (50% 20-year survival) while women with lobular breast cancer had comparatively worse survival (40% 20-year survival).
- Among women with lobular breast cancer, patient characteristics that were associated with worse survival include older age over 55 years, lowest income quintile, and increasing number of associated medical comorbidities. Cancer characteristics associated with worse survival included stage III and IV cancer, high-grade histology and estrogen and progesterone receptor-negativity.
Conclusions: Over time, the incidence of lobular breast cancer is increasing. Over a 30-year period, women with lobular breast cancer had worse survival than women with ductal or mixed ductal-lobular breast cancer, highlighting a need for more research and better treatments for lobular breast cancer.
Lay summary by David Lim, MD
P5-14-01 Transcriptomic insights into lobular breast cancer biology: a retrospective analysis of the MINDACT clinical trial
The biology of lobular breast cancer (ILC) can differ from the most common subtype, invasive ductal breast cancer (IDC), which is now officially referred to as “invasive breast carcinoma of no special type” (NST). To gain further insights into ILC, these investigators chose to re-analyze clinical and biological data from the previous MINDACT trial, which had evaluated use of the “MammaPrint” test as guidance for adjuvant chemotherapy in a large number of breast cancer patients. Three main advantages to using the MINDACT dataset were noted. First, all pathology samples were evaluated at a central facility to minimize variations among reviewers, since accurate pathological evaluation is important for differentiating ILC from NST. Second, both a clinical assessment (based on the patient’s staging) and a genomic assessment (based on the tumor’s genetic makeup) of the relapse risk, as well as actual survival data, were available for the MINDACT patients. Finally, biological tumor data (transcriptomic data, reflecting which genes were expressed in these tumors and to what extent) was also available.
The researchers had 3 main objectives for conducting the current study:
- to better understand the biological differences between ILC and NST, focusing on the most prevalent tumors expressing the estrogen receptor (ER) and not harboring HER2 amplification (i.e., ER+/HER2- tumors);
- to investigate whether so-called ‘classic ILC’ differs from other ILC variants; and
- to investigate whether biological differences could be identified between recurring and non-recurring ER+/HER2- ILC in the subgroup of patients having a low clinical and low genomic risk, since a significant proportion of these patients did relapse but were not expected to.
Regarding the first objective, the researchers found many differences between the two main subtypes, some of which had been previously described while others were new, and they considered that this kind of information will help provide a basis for individualizing treatment for ILC patients in the future. Regarding the second, they noted that while patients with “classic ILC” generally have a better survival than those with “non-classic ILC” (including the so-called “pleomorphic” ILC subtype), the differences detected between these variants at the transcriptomic level in this study were subtle. Regarding the final objective, their investigation of certain molecular “hallmarks” (related to apoptosis or programmed cell death, inflammatory response, hypoxia and oncogenic signaling) provided some insights as to why patients with ILC may have had recurrences despite having a favorable clinical and genomic risk assessment.
The researchers believe that this study represents the largest set of gene expression data for ILC patients to originate from a clinical trial where histology was reviewed centrally, and that the results have potential to personalize treatment for patients with ILC.
This project was funded by the Breast Cancer Research Foundation.
Lay summary by Christine Desmedt, PhD
P6-01-30 PgR levels and Ki67 expression of lobular carcinomas of the breast might indicate OncotypeDX testing to evaluate chemotherapy benefit
{kind=link}
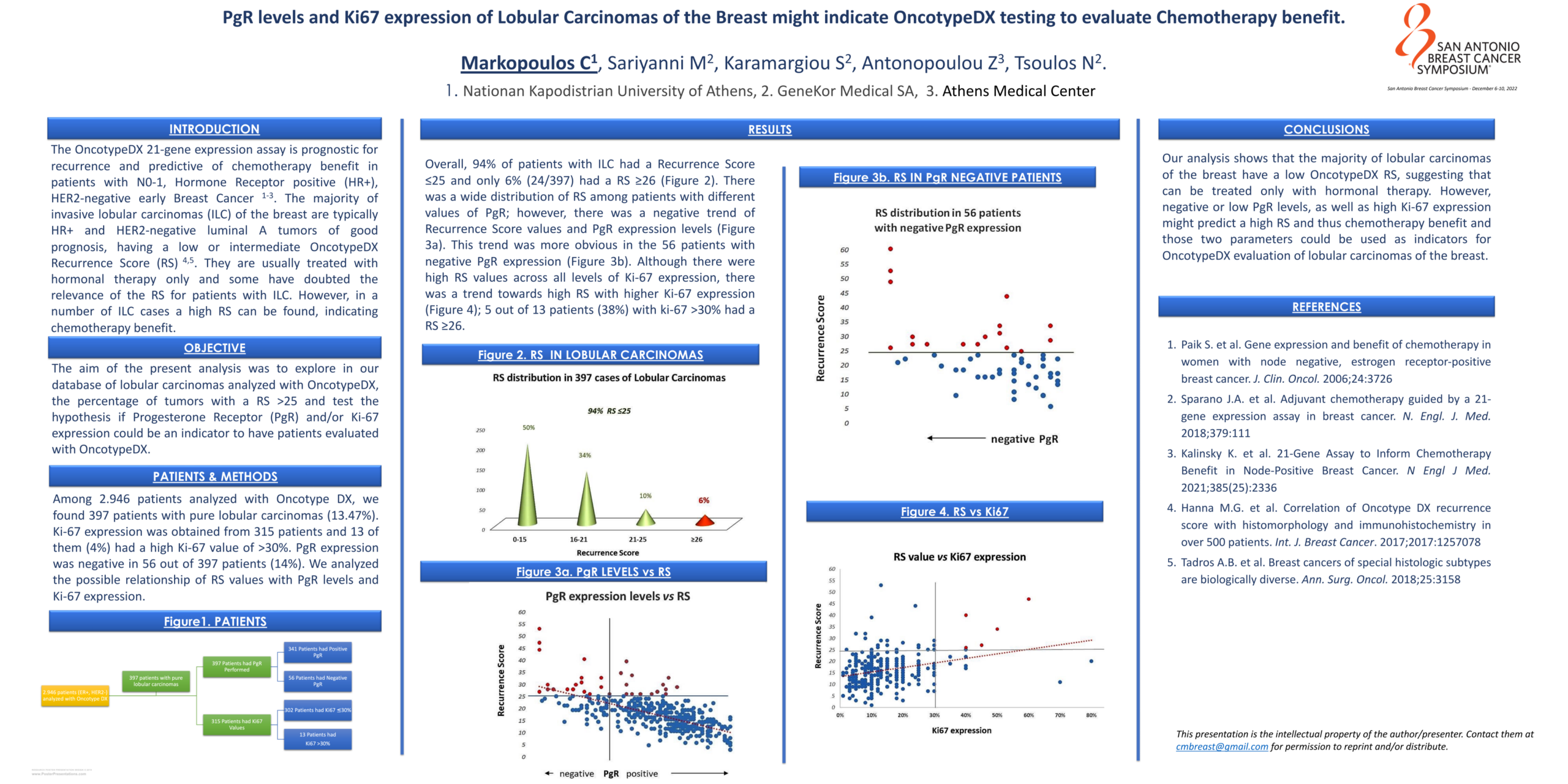
The OncotypeDX 21-gene expression assay is prognostic for recurrence and predictive of chemotherapy benefit in patients with N0-1, Hormone Receptor positive (HR+), HER2-negative early Breast Cancer. The majority of invasive lobular carcinomas (ILC) of the breast are typically HR+ and HER2-negative luminal A tumors of good prognosis, having a low or intermediate OncotypeDX Recurrence Score (RS). They are usually treated with hormonal therapy only and some have doubted the relevance of the RS for patients with ILC. However, in a number of ILC cases a high RS can be found, indicating chemotherapy benefit.
The aim of our study was to explore in our database of lobular carcinomas analyzed with OncotypeDX, the percentage of tumors with a RS >25 and test the hypothesis if Progesterone Receptor (PgR) and/or Ki-67 expression could be an indicator to have patients evaluated with OncotypeDX.
Among 2946 patients we found 397 patients with pure invasive lobular carcinomas (ILC) (13.5%). Ki-67 expression was obtained from 315 patients and 13 of them (4%) had a high Ki-67 value of >30%. PgR expression was low/negative in 56 out of 397 patients (14%).
- 94% of patients with ILC had a Recurrence Score ≤25 and only 6% (24/397) had a RS ≥26
- there was a wide distribution of RS among different values of PgR and Ki-67 expression
- there was a negative trend of RS values and PgR expression level: this was more obvious in the 56 patients with low/negative PgR expression: 31% of them had RS >25 compared to 6% in the total number of patients with ILC
- there was a trend towards high RS with higher Ki-67 expression; notably, 5 out of 13 patients with ki-67 >30% had a RS >25 (38%, compared to 6% in the total number of ILC).
In conclusion, our analysis shows that the majority of lobular carcinomas have a low OncotypeDX RS, suggesting that many can be treated only with hormonal therapy. However, negative or low PgR levels, as well as high Ki-67 expression might predict a high RS and thus chemotherapy benefit and those two parameters could be used as indicators for OncotypeDX evaluation of lobular carcinomas of the breast.
Lay summary by Christos Markopoulos, MD
P6-05-50 Lobular Breast Cancer Alliance Inc. Survey of Individuals with Metastatic Invasive Lobular Carcinoma
In June 2022, LBCA conducted an online survey of individuals diagnosed with metastatic ILC to hear about their experiences living with metastatic lobular breast disease. They were asked:
- Whether the metastatic diagnosis was de novo or a distant recurrence
- How their metastatic lobular breast disease was detected and where
- About progression, including the sites the lobular metastasis progressed to and whether a metastatic progression involved a change in receptor status
- About respondents’ experiences with non-oncologist clinicians and participation in clinical trials
There were 241 responses from women across the world. This included 77% of respondents from North America:
- 41% of respondents reported a de novo diagnosis, while 59% reported a distant recurrence.
- 48% reported their disease was found incidentally as part of a different medical work up.
- 36% reported at least one imaging modality failed to visualize their metastatic site.
- The most common metastatic site was bone, particularly for de novo diagnoses. 16% of metastases were to “unusual sites” including the eyes, skin, and organs of the reproductive and urinary systems.
- 47% of respondents experienced progression of their metastatic disease despite treatment, and only 28 women had participated in a clinical trial.
Results confirmed that a significant number of ILC patients present de novo with metastatic disease, and that better surveillance tools are desperately needed to detect these lobular cancers earlier. In addition, imaging modalities specific to ILC would help detect metastatic disease in unusual sites. Finally, more clinical trials and more opportunities for participation for patients with metastatic ILC are needed.
Lay summary by Laurie Hutcheson, MS
P6-08-09 Self-identified race and Area Deprivation Index in patients with invasive lobular carcinoma of the breast: associations with tumor characteristics and event free survival
A recent analysis of the The Surveillance, Epidemiology, and End Results (SEER) database showed that racial/ethnic identity is associated with worse outcomes in those with ILC. We wanted to validate these findings in our institutional database of ILC patients and investigate whether including socioeconomic factors, measured using the Area Deprivation Index (ADI), would influence the associations between race and outcomes.
On univariate analysis, black race, high area deprivation, and overweight/obese category body mass index (BMI) were each shown to reduce event free survival (EFS). In a multivariate analysis, however, overweight/obese category BMI remained the only significant factor associated with reduced EFS.
Our findings illustrate complex associations between many factors that impact breast cancer outcomes. Chiefly, our data suggests that the relationship between race and EFS was mitigated by ADI and obesity, suggesting that race is not an independent predictor of outcomes for ILC patients.
Lay summary by Mandeep Kaur, DO